
Search
- Page Path
- HOME > Search
Original Article
- Thyroid
- The Diagnostic Role of Repeated Biopsy of Thyroid Nodules with Atypia of Undetermined Significance with Architectural Atypia on Core-Needle Biopsy
- Hye Hyeon Moon, Sae Rom Chung, Young Jun Choi, Tae-Yon Sung, Dong Eun Song, Tae Yong Kim, Jeong Hyun Lee, Jung Hwan Baek
- Endocrinol Metab. 2024;39(2):300-309. Published online January 3, 2024
- DOI: https://doi.org/10.3803/EnM.2023.1818
- 464 View
- 31 Download
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader  ePub
ePub - Background
We aimed to evaluate the utility of repeat biopsy of thyroid nodules classified as atypia of undetermined significance with architectural atypia (IIIB) on core-needle biopsy (CNB).
Methods
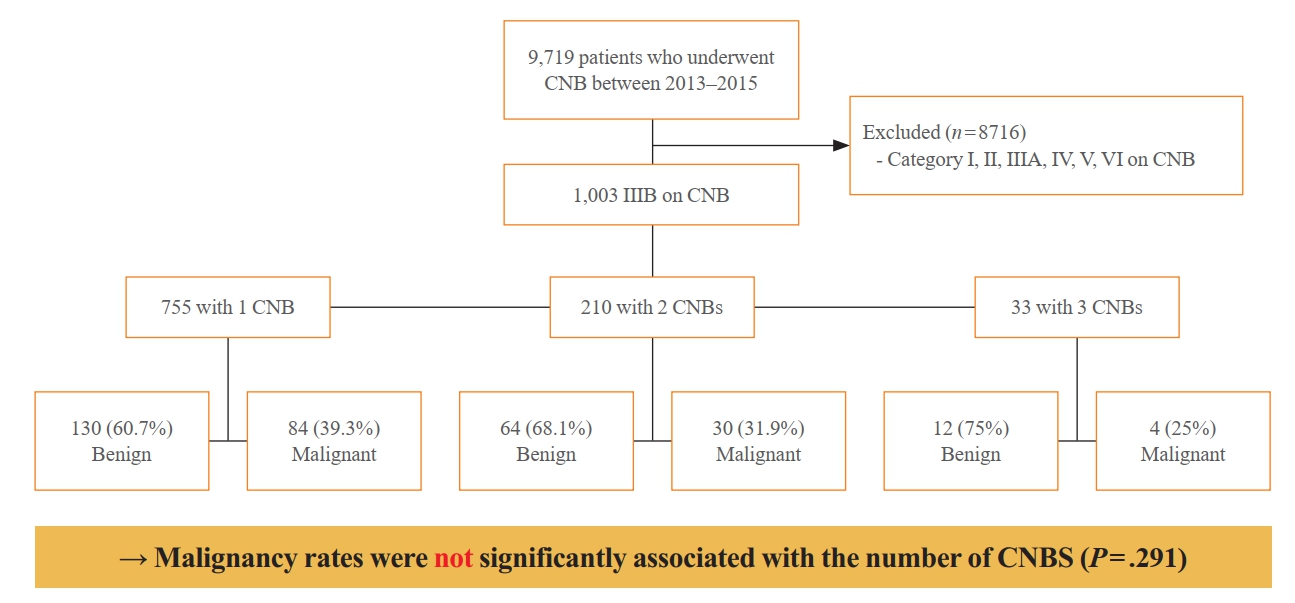
This retrospective study evaluated patients with thyroid nodules categorized as IIIB on CNB between 2013 and 2015. Demographic characteristics, subsequent biopsy results, and ultrasound (US) images were evaluated. The malignancy rates of nodules according to number of CNBs and the number of IIIB diagnoses was compared. Demographic and US features were evaluated to determine factors predictive of malignancy.
Results
Of 1,003 IIIB nodules on CNB, the final diagnosis was determined for 328 (32.7%) nodules, with 121 of them confirmed as malignant, resulting in a malignancy rate of 36.9% (95% confidence interval, 31.7% to 42.1%). Repeat CNB was performed in 248 nodules (24.7%), with 75 (30.2%), 131 (52.8%), 13 (5.2%), 26 (10.5%), one (0.4%), and two (0.8%) reclassified into categories II, IIIB, IIIA, IV, V, and VI, respectively. Malignancy rates were not significantly affected by the number of CNBs (P=0.291) or the number of IIIB diagnoses (P=0.473). None of the nodules confirmed as category II on repeat CNB was malignant. US features significantly associated with malignancy (P<0.003) included solid composition, irregular margins, microcalcifications, and high suspicion on the US risk stratification system.
Conclusion
Repeat biopsy of nodules diagnosed with IIIB on CNB did not increase the detection of malignancy but can potentially reduce unnecessary surgery. Repeat biopsy should be performed selectively, with US features guiding the choice between repeat biopsy and diagnostic surgery.

Editorial
- Thyroid
Thyroid Cancer Screening - Thyroid Cancer Screening: How to Maximize Its Benefits and Minimize Its Harms
- Jung Hwan Baek
- Endocrinol Metab. 2023;38(1):75-77. Published online February 27, 2023
- DOI: https://doi.org/10.3803/EnM.2023.105
- 1,254 View
- 112 Download
- 1 Web of Science
- 1 Crossref
Original Articles
- Clinical Study
- Effectiveness of Injecting Cold 5% Dextrose into Patients with Nerve Damage Symptoms during Thyroid Radiofrequency Ablation
- Min Kyoung Lee, Jung Hwan Baek, Sae Rom Chung, Young Jun Choi, Yu-Mi Lee, Tae Yong Kim, Jeong Hyun Lee
- Endocrinol Metab. 2020;35(2):407-415. Published online June 24, 2020
- DOI: https://doi.org/10.3803/EnM.2020.35.2.407

- 6,089 View
- 140 Download
- 12 Web of Science
- 14 Crossref
-
Abstract
PDFPubReader ePub
- Background
Although radiofrequency ablation (RFA) is a safe treatment for thyroid tumors, nerve damage is a frequent complication. A previous retrospective study suggested that an injection of cold 5% dextrose in water (5% DW) can reduce nerve damage during RFA. This study validated the efficacy of injecting cold 5% DW for management of nerve damage during RFA.
Methods
Between November 2017 and December 2018, 242 patients underwent 291 RFA sessions for treatment of benign thyroid nodules or recurrent thyroid cancers. Using a standardized technique, cold (0°C to 4°C) 5% DW was immediately injected around the damaged nerve into patients with any symptoms suggesting nerve damage. The incidence of nerve damage, the volume of 5% DW injected, symptom recovery time and the incidence of permanent nerve damage were evaluated.
Results
Nineteen patients experienced nerve damage symptoms related to 21 RFA sessions, including 17 patients during 19 sessions and two patients on the day after two sessions. Patients with nerve damage symptoms detected during RFA were treated by injection of a mean 41 mL (range, 3 to 260) cold 5% DW, but the two patients who experienced symptoms the next day did not receive cold 5% DW injections. Immediate recovery was observed after 15 RFA sessions in 14 patients. No patient experienced permanent nerve damage.
Conclusion
Injection of cold 5% DW is effective in managing nerve damage during RFA of thyroid lesions. -
Citations
Citations to this article as recorded by
- The Role of Radiofrequency Ablation in Benign and Malignant Thyroid Nodules
Meghal Shah, Catherine McManus
Surgical Clinics of North America.2024;[Epub] CrossRef - Clinical and Economic Evaluation of Ultrasound-Guided Radiofrequency Ablation vs. Parathyroidectomy for Patients with Primary Hyperparathyroidism: A Cohort Study
Hui-hui Chai, Zhan-jing Dai, Bai Xu, Qiao-hong Hu, Hong-feng He, Ying Xin, Wen-wen Yue, Cheng-zhong Peng
Academic Radiology.2023; 30(11): 2647. CrossRef - Efficacy of single-session radiofrequency ablation (RFA) in rendering euthyroidism for persistent/relapsed Graves’ disease, a pilot study
Man Him Matrix Fung, Brian Hung Hin Lang
European Radiology.2023; 33(9): 6534. CrossRef - Radiofrequency Ablation of Cervical Thyroid Cancer Metastases—Experience of Endocrinology Practices in the United States
Shahzad Ahmad, Jules Aljammal, Ian Orozco, Sheharyar Raashid, Fizza Zulfiqar, Sean P Nikravan, Iram Hussain
Journal of the Endocrine Society.2023;[Epub] CrossRef - Radiofrequency ablation of benign thyroid nodules: the value of anterolateral hydrodissection
So Yeong Jeong, Jung Hwan Baek, Sae Rom Chung, Young Jun Choi, Ki-Wook Chung, Tae Yong Kim, Jeong Hyun Lee
Ultrasonography.2023; 42(3): 432. CrossRef - Effective and Safe Application of Radiofrequency Ablation for Benign Thyroid Nodules
Jin Yong Sung
Journal of the Korean Society of Radiology.2023; 84(5): 985. CrossRef - Assessment of thyroid-specific quality of life in patients with benign symptomatic thyroid nodules treated with radiofrequency or ethanol ablation: a prospective multicenter study
So Yeong Jeong, Eun Ju Ha, Jung Hwan Baek, Tae Yong Kim, Yu-Mi Lee, Jeong Hyun Lee, Jeonghun Lee
Ultrasonography.2022; 41(1): 204. CrossRef - Management of Recurrent Laryngeal Nerve Injury During Radiofrequency Ablation of Thyroid Nodules
Jules Aljammal, Iram Hussain, Shahzad Ahmad
AACE Clinical Case Reports.2022; 8(2): 102. CrossRef - Thermal Ablation for the Management of Papillary Thyroid Microcarcinoma in the Era of Active Surveillance and Hemithyroidectomy
Sae Rom Chung, Jung Hwan Baek, Young Jun Choi, Jeong Hyun Lee
Current Oncology Reports.2022; 24(8): 1045. CrossRef - Improving Voice Outcomes after Thyroid Surgery and Ultrasound-Guided Ablation Procedures
Pia Pace-Asciak, Jon O. Russell, Ralph P. Tufano
Frontiers in Surgery.2022;[Epub] CrossRef - Using Intra‐Operative Laryngeal Ultrasonography as a Real‐Time Tool in Assessing Vocal Cord Function During Radiofrequency Ablation of the Thyroid Gland
Matrix Man Him Fung, Brian Hung Hin Lang
World Journal of Surgery.2022; 46(9): 2206. CrossRef - Long-term outcome of microwave ablation for benign thyroid nodules: Over 48-month follow-up study
Jia-Rui Du, Wen-Hui Li, Cheng-Hai Quan, Hui Wang, Deng-Ke Teng
Frontiers in Endocrinology.2022;[Epub] CrossRef - Continuous neuromonitoring during radiofrequency ablation of benign thyroid nodules provides objective evidence of laryngeal nerve safety
Catherine F. Sinclair, Maria J. Téllez, Roberto Peláez-Cruz, Alba Díaz-Baamonde, Sedat Ulkatan
The American Journal of Surgery.2021; 222(2): 354. CrossRef - Future Considerations and Directions for Thermal Ablative Technologies
Jonathon Russell, Catherine F. Sinclair
Current Otorhinolaryngology Reports.2021; 9(2): 210. CrossRef
- The Role of Radiofrequency Ablation in Benign and Malignant Thyroid Nodules
- Clinical Study
- Long-Term Results of Thermal Ablation of Benign Thyroid Nodules: A Systematic Review and Meta-Analysis
- Se Jin Cho, Jung Hwan Baek, Sae Rom Chung, Young Jun Choi, Jeong Hyun Lee
- Endocrinol Metab. 2020;35(2):339-350. Published online June 24, 2020
- DOI: https://doi.org/10.3803/EnM.2020.35.2.339

- 10,848 View
- 306 Download
- 39 Web of Science
- 45 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
Ultrasound-guided thermal ablations have become one of the main options for treating benign thyroid nodules. To determine efficacy of thermal ablation of benign thyroid nodules, we performed a meta-analysis of studies with long-term follow-up of more than 3 years.
Methods
Databases were searched for studies published up to August 25, 2019, reporting patients with benign thyroid nodules treated with thermal ablation and with follow-up data of more than 3 years. Data extraction and quality assessment were performed according to PRISMA guidelines. The analysis yielded serial volume reduction rates (VRRs) of ablated nodules for up to 3 years or more, and adverse effect of ablation during follow-up. Radiofrequency ablation (RFA) and laser ablation (LA) were compared in a subgroup analysis.
Results
The pooled VRRs for ablated nodules showed rapid volume reduction before 12 months, a plateau from 12 to 36 months, and more volume reduction appearing after 36 months, demonstrating long-term maintenance of treatment efficacy. Thermal ablation had an acceptable complication rate of 3.8%. Moreover, patients undergoing nodule ablation showed no unexpected delayed complications during the follow-up period. In the subgroup analysis, RFA was shown to be superior to LA in terms of the pooled VRR and the number of patients who underwent delayed surgery.
Conclusion
Thermal ablations are safe and effective methods for treating benign thyroid nodules, as shown by a long follow-up analysis of more than 3 years. In addition, RFA showed superior VRRs compared with LA for the treatment of benign thyroid nodules, with less regrowth and less delayed surgery. -
Citations
Citations to this article as recorded by- Five-year follow-up results of thermal ablation for benign thyroid nodules: Systematic review and meta-analysis
Xidong Xu, Ying Peng, Guoxin Han
American Journal of Otolaryngology.2024; 45(1): 104025. CrossRef - Radiofrequency Ablation for Benign Nodules and for Cancer, Too?
Jonathon O. Russell, Kaitlyn M. Frazier
Otolaryngologic Clinics of North America.2024; 57(1): 83. CrossRef - An anthropomorphic thyroid phantom for ultrasound‐guided radiofrequency ablation of nodules
Tim Boers, Wyger Brink, Leonardo Bianchi, Paola Saccomandi, Johan van Hespen, Germen Wennemars, Sicco Braak, Michel Versluis, Srirang Manohar
Medical Physics.2024; 51(2): 826. CrossRef - The safety and efficacy of radiofrequency ablation in benign pediatric thyroid disease in the US: An initial case series
Grace S. Kim, Hilary Seeley, Julia Noel, Iram Ahmad, Kara Meister
Laryngoscope Investigative Otolaryngology.2024;[Epub] CrossRef - Radioiodine versus radiofrequency ablation to treat autonomously functioning thyroid nodules: a systematic review and comparative meta-analysis
Luca Giovanella, Maria Luisa Garo, Alfredo Campenní, Petra Petranović Ovčariček
European Journal of Nuclear Medicine and Molecular Imaging.2024;[Epub] CrossRef - Novel and Advanced Ultrasound Techniques for Thyroid Thermal Ablation
Wai-Kin Chan, Jui-Hung Sun, Miaw-Jene Liou, Chia-Jung Hsu, Yu-Ling Lu, Wei-Yu Chou, Yan-Rong Li, Feng-Hsuan Liu
Endocrinology and Metabolism.2024; 39(1): 40. CrossRef - Sublethal thermal stress promotes migration and invasion of thyroid cancer cells
Chi-Yu Kuo, Chung-Hsin Tsai, Jun Kui Wu, Shih-Ping Cheng, Yi-Hsien Hsieh
PLOS ONE.2024; 19(2): e0298903. CrossRef - The Role of Radiofrequency Ablation in Benign and Malignant Thyroid Nodules
Meghal Shah, Catherine McManus
Surgical Clinics of North America.2024;[Epub] CrossRef - Comparison of ultrasound-guided microwave ablation, laser ablation, and radiofrequency ablation for the treatment of elderly patients with benign thyroid nodules: A meta-analysis
Ying Qian, Zheng Li, Chunyun Fan, Yong Huang
Experimental Gerontology.2024; 191: 112425. CrossRef - Ultrasound imaging in thyroid nodule diagnosis, therapy, and follow‐up: Current status and future trends
Tim Boers, Sicco J. Braak, Nicole E. T. Rikken, Michel Versluis, Srirang Manohar
Journal of Clinical Ultrasound.2023; 51(6): 1087. CrossRef - Ultrasound (US)-Guided Ablation of Thyroid Nodules
Byung Seup Kim
Journal of Surgical Ultrasound.2023; 10(1): 14. CrossRef - Ultrasound-Guided Radiofrequency Ablation versus Thyroidectomy for the Treatment of Benign Thyroid Nodules in Elderly Patients: A Propensity-Matched Cohort Study
L. Yan, X.Y. Li, Y. Li, Y. Luo
American Journal of Neuroradiology.2023; 44(6): 693. CrossRef - Minimally Invasive Ablative Treatments for Benign Thyroid Nodules: Current Evidence and Future Directions
Enrico Papini, Laszlo Hegedüs
Thyroid®.2023; 33(8): 890. CrossRef - Influence factors and nomogram for volume reduction rate in benign thyroid nodule after thermal ablation
Shiliang Cao, Lijia Wang, Ying Wei, Zhenlong Zhao, Jie Wu, Mingan Yu
International Journal of Hyperthermia.2023;[Epub] CrossRef - Choice in Ablative Therapies for Thyroid Nodules
Q Lina Hu, Jennifer H Kuo
Journal of the Endocrine Society.2023;[Epub] CrossRef - 2022 Taiwan clinical multicenter expert consensus and recommendations for thyroid radiofrequency ablation
Wei-Che Lin, Wen-Chieh Chen, Pei-Wen Wang, Yi-Chia Chan, Yen-Hsiang Chang, Harn-Shen Chen, Szu-Tah Chen, Wei-Chih Chen, Kai-Lun Cheng, Shun-Yu Chi, Pi-Ling Chiang, Chen-Kai Chou, Feng-Fu Chou, Shun-Chen Huang, Feng-Hsuan Liu, Sheng-Dean Luo, Fen-Yu Tseng,
Ultrasonography.2023; 42(3): 357. CrossRef - Comparison of the Efficiency of Radiofrequency and Microwave Ablation Methods in the Treatment of Benign Thyroid Nodules
Mahi N. Cerit, Cem Yücel, Ethem T. Cerit, Mehmet M. Yalçın, Halit N. Şendur, Suna Ö. Oktar
Academic Radiology.2023; 30(10): 2172. CrossRef - Radiofrequency ablation for autonomously functioning nodules as treatment for hyperthyroidism: subgroup analysis of toxic adenoma and multinodular goitre and predictors for treatment success
M. M. D. van der Meeren, F. B. M. Joosten, S. H. P. P. Roerink, L. N. Deden, W. J. G. Oyen
European Journal of Nuclear Medicine and Molecular Imaging.2023; 50(12): 3675. CrossRef - Massive Hemorrhage and Mortality Following Thyroid Radiofrequency Ablation
Seulki Song, Jin Pyeong Kim
Ear, Nose & Throat Journal.2023;[Epub] CrossRef - Clinical Approach for Thyroid Radiofrequency Ablation
Jung Suk Sim
Journal of the Korean Society of Radiology.2023; 84(5): 1017. CrossRef - General Principles for the Safe Performance, Training, and Adoption of Ablation Techniques for Benign Thyroid Nodules: An American Thyroid Association Statement
Catherine F. Sinclair, Jung Hwan Baek, Kathleen E. Hands, Steven P. Hodak, Timothy C. Huber, Iram Hussain, Brian Hung-Hin Lang, Julia E. Noel, Maria Papaleontiou, Kepal N. Patel, Gilles Russ, Jonathon Russell, Stefano Spiezia, Jennifer H. Kuo
Thyroid®.2023; 33(10): 1150. CrossRef - A comprehensive review of interventional ablation techniques for the management of thyroid nodules and metastatic lymph nodes
Jennifer H. Kuo, Catherine F. Sinclair, Brian Lang, Stefano Spiezia, Mingan Yu, Eun Ju Ha, Dong Gyu Na, Chiara Offi, Kepal N. Patel, Jung Hwan Baek
Surgery.2022; 171(4): 920. CrossRef - Radiofrequency ablation and related ultrasound‐guided ablation technologies for treatment of benign and malignant thyroid disease: An international multidisciplinary consensus statement of the American Head and Neck Society Endocrine Surgery Section with
Lisa A. Orloff, Julia E. Noel, Brendan C. Stack, Marika D. Russell, Peter Angelos, Jung Hwan Baek, Kevin T. Brumund, Feng‐Yu Chiang, Mary Beth Cunnane, Louise Davies, Andrea Frasoldati, Anne Y. Feng, Laszlo Hegedüs, Ayaka J. Iwata, Emad Kandil, Jennifer K
Head & Neck.2022; 44(3): 633. CrossRef - Assessment of thyroid-specific quality of life in patients with benign symptomatic thyroid nodules treated with radiofrequency or ethanol ablation: a prospective multicenter study
So Yeong Jeong, Eun Ju Ha, Jung Hwan Baek, Tae Yong Kim, Yu-Mi Lee, Jeong Hyun Lee, Jeonghun Lee
Ultrasonography.2022; 41(1): 204. CrossRef - Thyroid Nodule Radiofrequency Ablation: Complications and Clinical Follow Up
James Y. Lim, Jennifer H. Kuo
Techniques in Vascular and Interventional Radiology.2022; 25(2): 100824. CrossRef - Radiofrequency Ablation of Solid, Non-Functional Thyroid Nodules
Michael Douek
Techniques in Vascular and Interventional Radiology.2022; 25(2): 100821. CrossRef - Efficacy and Safety of Thermal Ablation for Treating Lymph Node Metastasis From Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis
Zheng Ding, Juan Chen, Zhiguang Chen, Xiaoke Zeng, Pengchao Zheng, Xuemei Wang, Xinwu Cui, Liang Sang
Frontiers in Oncology.2022;[Epub] CrossRef - Intraoperative Neuromonitoring: Evaluating the Role of Continuous IONM and IONM Techniques for Emerging Surgical and Percutaneous Procedures
Catherine McManus, Jennifer Hong Kuo
Frontiers in Endocrinology.2022;[Epub] CrossRef - Thermal Ablation for the Management of Papillary Thyroid Microcarcinoma in the Era of Active Surveillance and Hemithyroidectomy
Sae Rom Chung, Jung Hwan Baek, Young Jun Choi, Jeong Hyun Lee
Current Oncology Reports.2022; 24(8): 1045. CrossRef - enhanced anarchic society optimization technique for the classification of ultrasound thyroid images using ILBP
D. Anitha, S. Sathya Priya
International journal of health sciences.2022; : 4713. CrossRef - Image-Guided Percutaneous Ablation for Primary and Metastatic Tumors
Arian Mansur, Tushar Garg, Apurva Shrigiriwar, Vahid Etezadi, Christos Georgiades, Peiman Habibollahi, Timothy C. Huber, Juan C. Camacho, Sherif G. Nour, Alan Alper Sag, John David Prologo, Nariman Nezami
Diagnostics.2022; 12(6): 1300. CrossRef - Efficacy and safety of ultrasound-guided microwave ablation versus surgical resection for Bethesda category IV thyroid nodules: A retrospective comparative study
Jingjing Yang, Ya Zhang, Xingjia Li, Yueting Zhao, Xue Han, Guofang Chen, Xiaoqiu Chu, Ruiping Li, Jianhua Wang, Fei Huang, Chao Liu, Shuhang Xu
Frontiers in Endocrinology.2022;[Epub] CrossRef - Long-term follow-up of the radiofrequency ablation of benign thyroid nodules: the value of additional treatment
Hyun Jin Kim, Jung Hwan Baek, Woojin Cho, Jung Suk Sim
Ultrasonography.2022; 41(4): 661. CrossRef - Das „heiße“ Schilddrüsenkarzinom mit einem kritischen Blick auf die Thermoablation
Joachim Jähne, Andreas Niesen, Joachim Bernhardts, Marija Hillemans
Der Chirurg.2021; 92(1): 34. CrossRef - Current Practice of Percutaneous Ablation Technologies for Thyroid Nodules 2020
Haris Muhammad, Jonathon O. Russell, Prasanna Santhanam, Aniqa Tehreem, Ralph P. Tufano
Current Otorhinolaryngology Reports.2021; 9(1): 52. CrossRef - RFA and benign thyroid nodules: Review of the current literature
Haris Muhammad, Prasanna Santhanam, Jonathon O. Russell, Jennifer H. Kuo
Laryngoscope Investigative Otolaryngology.2021; 6(1): 155. CrossRef - Thermal Treatment Options for Benign Thyroid Nodules—The Role of Radio-Frequency Ablation and Laser Therapy
Erivelto Volpi
Clinical Thyroidology.2021; 33(1): 17. CrossRef - Comparative efficacy of different ultrasound-guided ablation for the treatment of benign thyroid nodules: Systematic review and network meta-analysis of randomized controlled trials
Linye He, Wanjun Zhao, Zijing Xia, Anping Su, Zhihui Li, Jingqiang Zhu, Ivan D. Florez
PLOS ONE.2021; 16(1): e0243864. CrossRef - Unresolved Clinical Issues in Thermal Ablation of Benign Thyroid Nodules: Regrowth at Long-Term Follow-Up
Jung Suk Sim, Jung Hwan Baek
Korean Journal of Radiology.2021; 22(8): 1436. CrossRef - Current Status and Challenges of US-Guided Radiofrequency Ablation of Thyroid Nodules in the Long Term: A Systematic Review
Stella Bernardi, Andrea Palermo, Rosario Francesco Grasso, Bruno Fabris, Fulvio Stacul, Roberto Cesareo
Cancers.2021; 13(11): 2746. CrossRef - Update of Radiofrequency Ablation for Treating Benign and Malignant Thyroid Nodules. The Future Is Now
Ralph P. Tufano, Pia Pace-Asciak, Jonathon O. Russell, Carlos Suárez, Gregory W. Randolph, Fernando López, Ashok R. Shaha, Antti Mäkitie, Juan P. Rodrigo, Luiz Paulo Kowalski, Mark Zafereo, Peter Angelos, Alfio Ferlito
Frontiers in Endocrinology.2021;[Epub] CrossRef - Factors Associated with the Efficacy of Radiofrequency Ablation in the Treatment of Benign Thyroid Nodules
Huynh Q Khanh, Nguyen L Vuong, Tran Q Tien
World Journal of Endocrine Surgery.2021; 12(3): 117. CrossRef - Long-Term Outcomes of Thermal Ablation for Benign Thyroid Nodules: The Issue of Regrowth
Jung Suk Sim, Jung Hwan Baek, Rosaria Meccariello
International Journal of Endocrinology.2021; 2021: 1. CrossRef - Matrix 3D ultrasound-assisted thyroid nodule volume estimation and radiofrequency ablation: a phantom study
T. Boers, S. J. Braak, M. Versluis, S. Manohar
European Radiology Experimental.2021;[Epub] CrossRef - Learning curve analysis of radiofrequency ablation for benign thyroid nodules
Chi-Yu Kuo, Chien-Liang Liu, Chung-Hsin Tsai, Shih-Ping Cheng
International Journal of Hyperthermia.2021; 38(1): 1536. CrossRef
- Five-year follow-up results of thermal ablation for benign thyroid nodules: Systematic review and meta-analysis
- Clinical Study
- Revisiting Rupture of Benign Thyroid Nodules after Radiofrequency Ablation: Various Types and Imaging Features
- Sae Rom Chung, Jung Hwan Baek, Jin Yong Sung, Ji Hwa Ryu, So Lyung Jung
- Endocrinol Metab. 2019;34(4):415-421. Published online December 23, 2019
- DOI: https://doi.org/10.3803/EnM.2019.34.4.415
- 5,800 View
- 96 Download
- 22 Web of Science
- 24 Crossref
-
Abstract
PDFPubReader ePub
Background To evaluate the imaging features, clinical manifestations, and prognosis of patients with thyroid nodule rupture after radiofrequency ablation (RFA).
Methods The records of 12 patients who experienced thyroid nodule rupture after RFA at four Korean thyroid centers between March 2010 and July 2017 were retrospectively reviewed. Clinical data evaluated included baseline patient characteristics, treatment methods, initial presenting symptoms, imaging features, treatment, and prognosis.
Results The most common symptoms of post-RFA nodule rupture were sudden neck bulging and pain. Based on imaging features, the localization of nodule rupture was classified into three types: anterior, posterolateral, and medial types. The anterior type is the most often, followed by posterolateral and medial type. Eight patients recovered completely after conservative treatment. Four patients who did not improve with conservative management required invasive procedures, including incision and drainage or aspiration.
Conclusion Thyroid nodule rupture after RFA can be classified into three types based on its localization: anterior, posterolateral, and medial types. Because majority of thyroid nodule ruptures after RFA can be managed conservatively, familiarity with these imaging features is essential in avoiding unnecessary imaging workup or invasive procedures.
-
Citations
Citations to this article as recorded by- Assessing the efficacy of thyroid nodule radiofrequency ablation using patient-reported outcome measures
Ege Akgun, Gustavo Romero-Velez, Eren Berber
Surgery.2024; 175(3): 654. CrossRef - The Comparison of Efficacy and Safety between Radiofrequency Ablation Alone and Ethanol Ablation Followed by Radiofrequency Ablation in the Treatment of Mixed Cystic and Solid Thyroid Nodule
Min Gang Jo, Min Kyoung Lee, Jae Ho Shin, Min Guk Seo, So Lyung Jung
Journal of the Korean Society of Radiology.2024;[Epub] CrossRef - Cutaneous fistula formation after thyroid nodule rupture: A rare complication after radiofrequency ablation
Amanda J. Bastien, Luv Amin, Jeffrey Moses, Wendy Sacks, Allen S. Ho
Head & Neck.2024;[Epub] CrossRef - Thyroid nodule rupture after radiofrequency ablation: case report and literature review
Tatiana Ferraro, Sameeha Sajid, Steven P. Hodak, Chelsey K. Baldwin
Frontiers in Endocrinology.2024;[Epub] CrossRef - Radiofrequency Ablation for Benign Thyroid Nodules: Radiology In Training
Ningcheng Li, Timothy C. Huber
Radiology.2023; 306(1): 54. CrossRef - A Case of Thyroid Abscess Following Ethanol Ablation for Benign Thyroid Nodule
Heungrae Cho, Dongbin Ahn, Ji Hye Kwak, Gil Joon Lee
Korean Journal of Otorhinolaryngology-Head and Neck Surgery.2023; 66(9): 624. CrossRef - Radiofrequency Ablation for Benign Thyroid Nodules
Julia E Noel, Catherine F Sinclair
The Journal of Clinical Endocrinology & Metabolism.2023; 109(1): e12. CrossRef - 2022 Taiwan clinical multicenter expert consensus and recommendations for thyroid radiofrequency ablation
Wei-Che Lin, Wen-Chieh Chen, Pei-Wen Wang, Yi-Chia Chan, Yen-Hsiang Chang, Harn-Shen Chen, Szu-Tah Chen, Wei-Chih Chen, Kai-Lun Cheng, Shun-Yu Chi, Pi-Ling Chiang, Chen-Kai Chou, Feng-Fu Chou, Shun-Chen Huang, Feng-Hsuan Liu, Sheng-Dean Luo, Fen-Yu Tseng,
Ultrasonography.2023; 42(3): 357. CrossRef - Effective and Safe Application of Radiofrequency Ablation for Benign Thyroid Nodules
Jin Yong Sung
Journal of the Korean Society of Radiology.2023; 84(5): 985. CrossRef - General Principles for the Safe Performance, Training, and Adoption of Ablation Techniques for Benign Thyroid Nodules: An American Thyroid Association Statement
Catherine F. Sinclair, Jung Hwan Baek, Kathleen E. Hands, Steven P. Hodak, Timothy C. Huber, Iram Hussain, Brian Hung-Hin Lang, Julia E. Noel, Maria Papaleontiou, Kepal N. Patel, Gilles Russ, Jonathon Russell, Stefano Spiezia, Jennifer H. Kuo
Thyroid®.2023; 33(10): 1150. CrossRef - Radiofrequency ablation and thyroid cancer: review of the current literature
Haris Muhammad, Aniqa Tehreem, Jonathon O. Russell
American Journal of Otolaryngology.2022; 43(1): 103204. CrossRef - Microwave Ablation Vs Traditional Thyroidectomy for Benign Thyroid Nodules: A Prospective, Non-Randomized Cohort Study
Shaokun Li, Mingfeng Yang, Haipeng Guo, Muyuan Liu, Shaowei Xu, Hanwei Peng
Academic Radiology.2022; 29(6): 871. CrossRef - Radiofrequency ablation and related ultrasound‐guided ablation technologies for treatment of benign and malignant thyroid disease: An international multidisciplinary consensus statement of the American Head and Neck Society Endocrine Surgery Section with
Lisa A. Orloff, Julia E. Noel, Brendan C. Stack, Marika D. Russell, Peter Angelos, Jung Hwan Baek, Kevin T. Brumund, Feng‐Yu Chiang, Mary Beth Cunnane, Louise Davies, Andrea Frasoldati, Anne Y. Feng, Laszlo Hegedüs, Ayaka J. Iwata, Emad Kandil, Jennifer K
Head & Neck.2022; 44(3): 633. CrossRef - Thyroid Nodule Radiofrequency Ablation: Complications and Clinical Follow Up
James Y. Lim, Jennifer H. Kuo
Techniques in Vascular and Interventional Radiology.2022; 25(2): 100824. CrossRef - Minimally-invasive treatments for benign thyroid nodules: recommendations for information to patients and referring physicians by the Italian Minimally-Invasive Treatments of the Thyroid group
Giovanni Mauri, Stella Bernardi, Andrea Palermo, Roberto Cesareo, Enrico Papini, Luigi Solbiati, Daniele Barbaro, Salvatore Monti, Maurilio Deandrea, Laura Fugazzola, Giovanni Gambelunghe, Roberto Negro, Stefano Spiezia, Fulvio Stacul, Luca Maria Sconfien
Endocrine.2022; 76(1): 1. CrossRef - American Association of Clinical Endocrinology Disease State Clinical Review: The Clinical Utility of Minimally Invasive Interventional Procedures in the Management of Benign and Malignant Thyroid Lesions
Sina Jasim, Kepal N. Patel, Gregory Randolph, Stephanie Adams, Roberto Cesareo, Edward Condon, Tara Henrichsen, Malak Itani, Maria Papaleontiou, Leonardo Rangel, John Schmitz, Marius N. Stan
Endocrine Practice.2022; 28(4): 433. CrossRef - Radiofrequency Ablation of Benign and Malignant Thyroid Nodules
Patrick J. Navin, Scott M. Thompson, Anil N. Kurup, Robert A. Lee, Matthew R. Callstrom, M. Regina Castro, Marius N. Stan, Brian T. Welch, John J. Schmitz
RadioGraphics.2022; 42(6): 1812. CrossRef - SFE-AFCE-SFMN 2022 consensus on the management of thyroid nodules: Thermal ablation
Adrien Ben Hamou, Edouard Ghanassia, Arnaud Muller, Miriam Ladsous, Nunzia Cinzia Paladino, Laurent Brunaud, Laurence Leenhardt, Gilles Russ
Annales d'Endocrinologie.2022; 83(6): 423. CrossRef - Complications of RFA for Thyroid Nodules: Prevention and Management
Rahul K. Sharma, Jennifer H Kuo
Current Otorhinolaryngology Reports.2021; 9(1): 79. CrossRef - Ultrasonographic characteristics of thyroid nodule rupture after microwave ablation
Peng Tian, Wenyan Du, Xiaoxi Liu, Yiwen Ding, Zekai Zhang, Jing Li, Yanzhen Wang
Medicine.2021; 100(9): e25070. CrossRef - Symptomatic aseptic necrosis of benign thyroid lesions after microwave ablation: risk factors and clinical significance
Jian-ping Dou, Jie Yu, Zhi-gang Cheng, Fang-yi Liu, Xiao-ling Yu, Qi-di Hou, Fang Liu, Zhi-yu Han, Ping Liang
International Journal of Hyperthermia.2021; 38(1): 815. CrossRef - The Importance of Nodule Size in the Management of Ruptured Thyroid Nodule After Radiofrequency Ablation: A Retrospective Study and Literature Review
Wen-Chieh Chen, Sheng-Dean Luo, Wei-Chih Chen, Chen-Kai Chou, Yen-Hsiang Chang, Kai-Lun Cheng, Wei-Che Lin
Frontiers in Endocrinology.2021;[Epub] CrossRef - Long-Term Follow-Up of Single-Fiber Multiple Low-Intensity Energy Laser Ablation Technique of Benign Thyroid Nodules
Mattia Squarcia, Mireia Mora, Gloria Aranda, Enrique Carrero, Daniel Martínez, Ramona Jerez, Ricard Valero, Joan Berenguer, Irene Halperin, Felicia A. Hanzu
Frontiers in Oncology.2021;[Epub] CrossRef - Effectiveness of Injecting Cold 5% Dextrose into Patients with Nerve Damage Symptoms during Thyroid Radiofrequency Ablation
Min Kyoung Lee, Jung Hwan Baek, Sae Rom Chung, Young Jun Choi, Yu-Mi Lee, Tae Yong Kim, Jeong Hyun Lee
Endocrinology and Metabolism.2020; 35(2): 407. CrossRef
- Assessing the efficacy of thyroid nodule radiofrequency ablation using patient-reported outcome measures
Response
- Thyroid
- Response: Long-Term Outcomes Following Thermal Ablation of Benign Thyroid Nodules as an Alternative to Surgery: The Importance of Controlling Regrowth (Endocrinol Metab 2019;34:117–23, Jung Suk Sim et al.)
- Jung Suk Sim, Jung Hwan Baek
- Endocrinol Metab. 2019;34(3):325-326. Published online September 26, 2019
- DOI: https://doi.org/10.3803/EnM.2019.34.3.325
- [Original]
- 3,527 View
- 45 Download
- 1 Web of Science
- 2 Crossref
-
PDFPubReader ePub
-
Citations
Citations to this article as recorded by- Five-year follow-up results of thermal ablation for benign thyroid nodules: Systematic review and meta-analysis
Xidong Xu, Ying Peng, Guoxin Han
American Journal of Otolaryngology.2024; 45(1): 104025. CrossRef - How to Monitor and Manage Nodule Regrowth after Thermal Ablation of Benign Thyroid Nodules
Sang Ik Park, Jung Hwan Baek
Korean Journal of Radiology.2021; 22(2): 293. CrossRef
- Five-year follow-up results of thermal ablation for benign thyroid nodules: Systematic review and meta-analysis
Review Article
- Thyroid
- Long-Term Outcomes Following Thermal Ablation of Benign Thyroid Nodules as an Alternative to Surgery: The Importance of Controlling Regrowth
- Jung Suk Sim, Jung Hwan Baek
- Endocrinol Metab. 2019;34(2):117-123. Published online June 24, 2019
- DOI: https://doi.org/10.3803/EnM.2019.34.2.117
- 9,936 View
- 150 Download
- 58 Web of Science
- 61 Crossref
-
Abstract
PDFPubReader ePub
Thermal ablation (TA) procedures, such as radiofrequency ablation and laser ablation, are used for the treatment of benign thyroid nodules. Short-term studies (<2 years) have demonstrated that TA is an effective and safe procedure to improve cosmetic or symptomatic problems. However, studies including a longer follow-up period show that treated thyroid nodules can increase in size after 2 to 3 years. Several studies suggest that this results from regrowth at the undertreated nodule margins. Here, we review current data on regrowth after TA and describe factors related to it and possible approaches to prevent it.
-
Citations
Citations to this article as recorded by- From ablation to operation: Unraveling the surgical outcomes and complications of thyroidectomy after radiofrequency ablation
Mohammad Hussein, Eman Toraih, Peter P. Issa, Mahmoud Omar, Mohamed Aboueisha, Yusef Buti, Chad P. Issa, Aaron L. Albuck, Katherine Cironi, Abdallah S. Attia, Alexandra C. LaForteza, Mohamed Shama, Emad Kandil
Surgery.2024; 175(1): 146. CrossRef - Radiofrequency Ablation for Benign Nodules and for Cancer, Too?
Jonathon O. Russell, Kaitlyn M. Frazier
Otolaryngologic Clinics of North America.2024; 57(1): 83. CrossRef - Clinical Outcomes of Thermal Ablation Re-Treatment of Benign Thyroid Nodules: A Multicenter Study from the Italian Minimally Invasive Treatments of the Thyroid Group
Stella Bernardi, Valentina Rosolen, Fabio Barbone, Stefano Borgato, Maurilio Deandrea, Pierpaolo De Feo, Laura Fugazzola, Giovanni Gambelunghe, Roberto Negro, Salvatore Oleandri, Giampaolo Papi, Enrico Papini, Francesca Retta, Ruth Rossetto, Daniela Sanso
Thyroid®.2024; 34(3): 360. CrossRef - An anthropomorphic thyroid phantom for ultrasound‐guided radiofrequency ablation of nodules
Tim Boers, Wyger Brink, Leonardo Bianchi, Paola Saccomandi, Johan van Hespen, Germen Wennemars, Sicco Braak, Michel Versluis, Srirang Manohar
Medical Physics.2024; 51(2): 826. CrossRef - The safety and efficacy of radiofrequency ablation in benign pediatric thyroid disease in the US: An initial case series
Grace S. Kim, Hilary Seeley, Julia Noel, Iram Ahmad, Kara Meister
Laryngoscope Investigative Otolaryngology.2024;[Epub] CrossRef - Comparison of the Therapeutic Efficacy and Technical Outcomes between Conventional Fixed Electrodes and Adjustable Electrodes in the Radiofrequency Ablation of Benign Thyroid Nodules
Jae Ho Shin, Minkook Seo, Min Kyoung Lee, So Lyung Jung
Korean Journal of Radiology.2024; 25(2): 199. CrossRef - Comparison of efficacy and safety of different minimally invasive therapies for thyroid nodules: A network meta-analysis
Wei Yuan, Liju Di, Xiaoxin Yu, Jian Li
Endocrine.2024;[Epub] CrossRef - If the price is right: Cost-effectiveness of radiofrequency ablation versus thyroidectomy in the treatment of benign thyroid nodules
Eric J. Kuo, Aaron Oh, Yinin Hu, Catherine M. McManus, James A. Lee, Jennifer H. Kuo
Surgery.2023; 173(1): 201. CrossRef - Development and validation of a nomogram model for predicting residue of partially cystic thyroid nodules after ultrasound-guided ethanol and thermal ablation
Di Li, Xiaoer Zhang, Yutong Zhang, Tongyi Huang, Rui Zhang, Wenwen Zhou, Xiaoyan Xie, Ming Xu
Frontiers in Endocrinology.2023;[Epub] CrossRef - Image-guided Thermal Ablation as a Promising Approach to Both Nontoxic and Toxic Autonomously Functioning Thyroid Nodules
Long Wang, Peiqing Wang, Zhijiang Chen, Yinghe Lin, Yingshan Liu, Rong Peng, Jinlian Li, Wenfeng Luo, Jian Kuang
Academic Radiology.2023; 30(11): 2636. CrossRef - Analysis and prediction of regrowth in benign thyroid nodules undergoing radiofrequency ablation: a retrospective study with a 5-year follow-up
Yi Li, Wen Li, Bo Jiang, Jiahang Zhao, Yan Zhang, Yukun Luo
European Radiology.2023; 33(8): 5615. CrossRef - Ultrasound (US)-Guided Ablation of Thyroid Nodules
Byung Seup Kim
Journal of Surgical Ultrasound.2023; 10(1): 14. CrossRef - Minimally Invasive Ablative Treatments for Benign Thyroid Nodules: Current Evidence and Future Directions
Enrico Papini, Laszlo Hegedüs
Thyroid®.2023; 33(8): 890. CrossRef - Ultrasound imaging in thyroid nodule diagnosis, therapy, and follow‐up: Current status and future trends
Tim Boers, Sicco J. Braak, Nicole E. T. Rikken, Michel Versluis, Srirang Manohar
Journal of Clinical Ultrasound.2023; 51(6): 1087. CrossRef - Radiofrequency ablation of benign thyroid nodules: the value of anterolateral hydrodissection
So Yeong Jeong, Jung Hwan Baek, Sae Rom Chung, Young Jun Choi, Ki-Wook Chung, Tae Yong Kim, Jeong Hyun Lee
Ultrasonography.2023; 42(3): 432. CrossRef - Radiofrequency Ablation for Benign Thyroid Nodules
Julia E Noel, Catherine F Sinclair
The Journal of Clinical Endocrinology & Metabolism.2023; 109(1): e12. CrossRef - High-security automatic path planning of radiofrequency ablation for liver tumors
Jing Li, Huayu Gao, Nanyan Shen, Di Wu, Lanyun Feng, Peng Hu
Computer Methods and Programs in Biomedicine.2023; 242: 107769. CrossRef - General Principles for the Safe Performance, Training, and Adoption of Ablation Techniques for Benign Thyroid Nodules: An American Thyroid Association Statement
Catherine F. Sinclair, Jung Hwan Baek, Kathleen E. Hands, Steven P. Hodak, Timothy C. Huber, Iram Hussain, Brian Hung-Hin Lang, Julia E. Noel, Maria Papaleontiou, Kepal N. Patel, Gilles Russ, Jonathon Russell, Stefano Spiezia, Jennifer H. Kuo
Thyroid®.2023; 33(10): 1150. CrossRef - Clinical Approach for Thyroid Radiofrequency Ablation
Jung Suk Sim
Journal of the Korean Society of Radiology.2023; 84(5): 1017. CrossRef - Contrast-enhanced ultrasound is a reliable and reproducible assessment of necrotic ablated volume after radiofrequency ablation for benign thyroid nodules: a retrospective study
Lin Yan, XinYang Li, Jing Xiao, YingYing Li, Yaqiong Zhu, Hongying He, Yukun Luo
International Journal of Hyperthermia.2022; 39(1): 40. CrossRef - Nonsurgical Management of Thyroid Nodules: The Role of Ablative Therapies
Marius N Stan, Maria Papaleontiou, John J Schmitz, M Regina Castro
The Journal of Clinical Endocrinology & Metabolism.2022; 107(5): 1417. CrossRef - Safety and Efficacy of Ultrasound-Guided Radiofrequency Ablation for Benign Nonfunctional Thyroid Nodules in Children: A Retrospective Study of 62 Patients with Over Four Years of Follow-Up
Liwen Li, Xinguang Qiu
Thyroid.2022; 32(5): 525. CrossRef - A Nomogram to Predict Regrowth After Ultrasound-Guided Radiofrequency Ablation for Benign Thyroid Nodules
Lin Yan, Mingbo Zhang, Xinyang Li, YingYing Li, Yukun Luo
Frontiers in Endocrinology.2022;[Epub] CrossRef - Radiofrequency Ablation of Solid, Non-Functional Thyroid Nodules
Michael Douek
Techniques in Vascular and Interventional Radiology.2022; 25(2): 100821. CrossRef - American Association of Clinical Endocrinology Disease State Clinical Review: The Clinical Utility of Minimally Invasive Interventional Procedures in the Management of Benign and Malignant Thyroid Lesions
Sina Jasim, Kepal N. Patel, Gregory Randolph, Stephanie Adams, Roberto Cesareo, Edward Condon, Tara Henrichsen, Malak Itani, Maria Papaleontiou, Leonardo Rangel, John Schmitz, Marius N. Stan
Endocrine Practice.2022; 28(4): 433. CrossRef - The Use of Radiofrequency Ablation for Benign Thyroid Nodules
Rachel Liou, Catherine McManus, Jennifer Kuo
VideoEndocrinology.2022; 9(2): 36. CrossRef - A novel parallel overlapping mode for complete ablation of large benign thyroid nodules in a single-session radiofrequency ablation
Tao Wu, Bowen Zheng, Lei Tan, Tinghui Yin, Yufan Lian, Shicheng Xu, Jin Ye, Jie Ren
Frontiers in Endocrinology.2022;[Epub] CrossRef - Efficacy and safety of thermal ablation for autonomously functioning thyroid nodules: a systematic review and meta-analysis
Hyun Jin Kim, Se Jin Cho, Jung Hwan Baek, Chong Hyun Suh
European Radiology.2021; 31(2): 605. CrossRef - Letter: Twelve-Month Volume Reduction Ratio Predicts Regrowth and Time to Regrowth in Thyroid Nodules Submitted to Laser Ablation: A 5-Year Follow-Up Retrospective Study
Jung Suk Sim
Korean Journal of Radiology.2021; 22(2): 291. CrossRef - How to Monitor and Manage Nodule Regrowth after Thermal Ablation of Benign Thyroid Nodules
Sang Ik Park, Jung Hwan Baek
Korean Journal of Radiology.2021; 22(2): 293. CrossRef - Non-enhanced ultrasound is not a satisfactory modality for measuring necrotic ablated volume after radiofrequency ablation of benign thyroid nodules: a comparison with contrast-enhanced ultrasound
Lin Yan, Yukun Luo, Jing Xiao, Lin Lin
European Radiology.2021; 31(5): 3226. CrossRef - The Adoption of Ultrasound-guided Radiofrequency Ablation of Thyroid Nodules in the United States
Jennifer H. Kuo, James A. Lee
Annals of Surgery.2021; 273(1): e10. CrossRef - Radiofrequency ablation of benign thyroid nodules: recommendations from the Asian Conference on Tumor Ablation Task Force
Eun Ju Ha, Jung Hwan Baek, Ying Che, Yi-Hong Chou, Nobuhiro Fukunari, Ji-hoon Kim, Wei-Che Lin, Le Thi My, Dong Gyu Na, Lawrence Han Hwee Quek, Ming-Hsun Wu, Koichiro Yamakado, Jianhua Zhou
Ultrasonography.2021; 40(1): 75. CrossRef - Thermal Treatment Options for Benign Thyroid Nodules—The Role of Radio-Frequency Ablation and Laser Therapy
Erivelto Volpi
Clinical Thyroidology.2021; 33(1): 17. CrossRef - Residual vital ratio predicts 5-year volume reduction and retreatment after radiofrequency ablation of benign thyroid nodules but not regrowth
Stella Bernardi, Fabiola Giudici, Giacomo Colombin, Marco Cavallaro, Fulvio Stacul, Bruno Fabris
International Journal of Hyperthermia.2021; 38(1): 111. CrossRef - Radiofrequency ablation versus reoperation for benign thyroid nodules that developed after previous thyroid surgery
Lin Yan, Cuiai Deng, Qing Song, Nan Li, Ling Ren, HongYing He, Wen Li, Mingbo Zhang, Yukun Luo
International Journal of Hyperthermia.2021; 38(1): 176. CrossRef - Letter to the Editor Regarding “Minimally Invasive Treatment for Benign Parathyroid Lesions: Treatment Efficacy and Safety Based on Nodule Characteristics”
Jung Suk Sim
Korean Journal of Radiology.2021; 22(5): 861. CrossRef - Unresolved Clinical Issues in Thermal Ablation of Benign Thyroid Nodules: Regrowth at Long-Term Follow-Up
Jung Suk Sim, Jung Hwan Baek
Korean Journal of Radiology.2021; 22(8): 1436. CrossRef - Current Status and Challenges of US-Guided Radiofrequency Ablation of Thyroid Nodules in the Long Term: A Systematic Review
Stella Bernardi, Andrea Palermo, Rosario Francesco Grasso, Bruno Fabris, Fulvio Stacul, Roberto Cesareo
Cancers.2021; 13(11): 2746. CrossRef - Long-Term Outcomes of Radiofrequency Ablation for Treatment of Cystic Warthin Tumors versus Solid Warthin Tumors
Chih-Hung Cha, Sheng-Dean Luo, Pi-Ling Chiang, Wei-Chih Chen, Yu-Cheng Tung, Yan-Ye Su, Wei-Che Lin
International Journal of Environmental Research and Public Health.2021; 18(12): 6640. CrossRef - Comparison of Thermal Ablation and Surgery for Low-Risk Papillary Thyroid Microcarcinoma: A Systematic Review and Meta-Analysis
Hyun Jin Kim, Se Jin Cho, Jung Hwan Baek
Korean Journal of Radiology.2021; 22(10): 1730. CrossRef - Long-Term Outcomes of Thermal Ablation for Benign Thyroid Nodules: The Issue of Regrowth
Jung Suk Sim, Jung Hwan Baek, Rosaria Meccariello
International Journal of Endocrinology.2021; 2021: 1. CrossRef - Matrix 3D ultrasound-assisted thyroid nodule volume estimation and radiofrequency ablation: a phantom study
T. Boers, S. J. Braak, M. Versluis, S. Manohar
European Radiology Experimental.2021;[Epub] CrossRef - Ultrasound-Guided Thermal Ablation of Bethesda IV Thyroid Nodules: A Pilot Study
Xinyang Li, Yu Lan, Nan Li, Lin Yan, Jing Xiao, Mingbo Zhang, Yukun Luo
Frontiers in Endocrinology.2021;[Epub] CrossRef - Percutaneous Microwave Ablation for Benign, Symptomatic Thyroid Nodules: Wave of the Future?
Alaina D. Geary, Frederick Thurston Drake
World Journal of Surgery.2020; 44(7): 2280. CrossRef - Radiofrequency Ablation Systemization
Leonardo Guimarães Rangel, Erivelto Martinho Volpi, Jose Higino Steck, Jonathon O. Russell, Ralph P. Tufano
VideoEndocrinology.2020;[Epub] CrossRef - Twelve-Month Volume Reduction Ratio Predicts Regrowth and Time to Regrowth in Thyroid Nodules Submitted to Laser Ablation: A 5-Year Follow-Up Retrospective Study
Roberto Negro, Gabriele Greco, Maurilio Deandrea, Matteo Rucco, Pierpaolo Trimboli
Korean Journal of Radiology.2020; 21(6): 764. CrossRef - Long-Term Results of Thermal Ablation of Benign Thyroid Nodules: A Systematic Review and Meta-Analysis
Se Jin Cho, Jung Hwan Baek, Sae Rom Chung, Young Jun Choi, Jeong Hyun Lee
Endocrinology and Metabolism.2020; 35(2): 339. CrossRef - Effectiveness of Injecting Cold 5% Dextrose into Patients with Nerve Damage Symptoms during Thyroid Radiofrequency Ablation
Min Kyoung Lee, Jung Hwan Baek, Sae Rom Chung, Young Jun Choi, Yu-Mi Lee, Tae Yong Kim, Jeong Hyun Lee
Endocrinology and Metabolism.2020; 35(2): 407. CrossRef - Vital volume increase versus clinical evaluation as the indication of additional radiofrequency ablation for benign thyroid nodule: a single center retrospective study
Lin Yan, Yukun Luo, Mingbo Zhang, Jing Xiao
International Journal of Hyperthermia.2020; 37(1): 777. CrossRef - Five-Year Results of Radiofrequency and Laser Ablation of Benign Thyroid Nodules: A Multicenter Study from the Italian Minimally Invasive Treatments of the Thyroid Group
Stella Bernardi, Fabiola Giudici, Roberto Cesareo, Giovanni Antonelli, Marco Cavallaro, Maurilio Deandrea, Massimo Giusti, Alberto Mormile, Roberto Negro, Andrea Palermo, Enrico Papini, Valerio Pasqualini, Bruno Raggiunti, Duccio Rossi, Luca Maria Sconfie
Thyroid.2020; 30(12): 1759. CrossRef - A practical pretreatment planning method of multiple puncturing for thermal ablation surgery
Jing Li, Yuanqi Xu, Nanyan Shen, Lanyun Feng, Zhuang Ran, Zongqian Deng
Biocybernetics and Biomedical Engineering.2020; 40(4): 1469. CrossRef - Radiofrequency for benign and malign thyroid lesions
Leonardo Rangel, Leonardo M. Volpi, Elaine Stabenow, Jose Higino Steck, Erivelto Volpi, Jonathon O. Russell, Ralph P. Tufano
World Journal of Otorhinolaryngology - Head and Neck Surgery.2020; 6(3): 188. CrossRef - Residual vital ratio: predicting regrowth after radiofrequency ablation for benign thyroid nodules
Lin Yan, Yukun Luo, Fang Xie, Mingbo Zhang, Jing Xiao
International Journal of Hyperthermia.2020; 37(1): 1139. CrossRef - Thermal Ablation of Benign Thyroid Nodules and Papillary Thyroid Microcarcinoma
Xiao-Wan Bo, Feng Lu, Hui-Xiong Xu, Li-Ping Sun, Kun Zhang
Frontiers in Oncology.2020;[Epub] CrossRef - Inter-observer reliability in ultrasound measurement of benign thyroid nodules in the follow-up of radiofrequency ablation: a retrospective study
Lin Yan, Yukun Luo, Qing Song, Nan Li, Jing Xiao, Ying Zhang, Yaqiong Zhu
International Journal of Hyperthermia.2020; 37(1): 1336. CrossRef - CT-based quantitative evaluation of the efficacy after radiofrequency ablation in patients with benign thyroid nodules
Yangsean Choi, So-Lyung Jung, Jinhee Jang, Na-Young Shin, Kook-Jin Ahn, Bum-soo Kim
International Journal of Hyperthermia.2020; 37(1): 742. CrossRef - 2020 European Thyroid Association Clinical Practice Guideline for the Use of Image-Guided Ablation in Benign Thyroid Nodules
Enrico Papini, Hervé Monpeyssen, Andrea Frasoldati, Laszlo Hegedüs
European Thyroid Journal.2020; 9(4): 172. CrossRef - Efficacy of Percutaneous Thermal Ablation of Papillary Thyroid Carcinoma
Ettore Caruso, Ettore Gagliano, Gianlorenzo Dionigi
Journal of Endocrine Surgery.2019; 19(4): 154. CrossRef - Response: Long-Term Outcomes Following Thermal Ablation of Benign Thyroid Nodules as an Alternative to Surgery: The Importance of Controlling Regrowth (Endocrinol Metab 2019;34:117–23, Jung Suk Sim et al.)
Jung Suk Sim, Jung Hwan Baek
Endocrinology and Metabolism.2019; 34(3): 325. CrossRef - Letter: Long-Term Outcomes Following Thermal Ablation of Benign Thyroid Nodules as an Alternative to Surgery: The Importance of Controlling Regrowth (Endocrinol Metab 2019;34:117-23, Jung Suk Sim et al.)
Tae Yong Kim
Endocrinology and Metabolism.2019; 34(3): 323. CrossRef
- From ablation to operation: Unraveling the surgical outcomes and complications of thyroidectomy after radiofrequency ablation
Original Articles
- Clinical Study
- Does Radiofrequency Ablation Induce Neoplastic Changes in Benign Thyroid Nodules: A Preliminary Study
- Su Min Ha, Jun Young Shin, Jung Hwan Baek, Dong Eun Song, Sae Rom Chung, Young Jun Choi, Jeong Hyun Lee
- Endocrinol Metab. 2019;34(2):169-178. Published online May 15, 2019
- DOI: https://doi.org/10.3803/EnM.2019.34.2.169
- 5,631 View
- 81 Download
- 20 Web of Science
- 19 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
Background To evaluate the clinical feasibility of radiofrequency ablation (RFA) of benign thyroid nodules along with cytomorphological alteration, and any malignant transformation through biopsy.
Methods The data were retrospectively collected between April 2008 and June 2013 and core needle biopsy (CNB) was performed on 16 benign thyroid nodules previously treated using RFA. The parameters of the patients were compared, between the time of enrollment and the last follow-up examination, using linear mixed model statistical analysis.
Results No atypical cells or neoplastic transformation were detected in the undertreated peripheral portion of treated benign nodules on the CNB specimen. RFA altered neither the thyroid capsule nor the thyroid tissue adjacent to the treated area. On histopathological examinations, we observed 81.2% acellular hyalinization, which was the most common finding. After a mean follow-up period of over 5 years, the mean volume of thyroid nodule had decreased to 6.4±4.2 mL, with a reduction rate of 81.3%±5.8% (
P <0.0001).Conclusion RFA is a technically feasible treatment method for benign thyroid nodules, with no carcinogenic effect or tissue damage of the normal thyroid tissue adjacent to the RFA-treated zone.
-
Citations
Citations to this article as recorded by- Comparison of the Therapeutic Efficacy and Technical Outcomes between Conventional Fixed Electrodes and Adjustable Electrodes in the Radiofrequency Ablation of Benign Thyroid Nodules
Jae Ho Shin, Minkook Seo, Min Kyoung Lee, So Lyung Jung
Korean Journal of Radiology.2024; 25(2): 199. CrossRef - Thermoablation of thyroid nodules reveals excellent results with low morbidity
Robert M. Eisele, Philipp R. Scherber, Monika Schlüter, Thorsten Drews, Matthias Glanemann, Gereon Gäbelein
Technology and Health Care.2022; 30(3): 683. CrossRef - Radiofrequency ablation and related ultrasound‐guided ablation technologies for treatment of benign and malignant thyroid disease: An international multidisciplinary consensus statement of the American Head and Neck Society Endocrine Surgery Section with
Lisa A. Orloff, Julia E. Noel, Brendan C. Stack, Marika D. Russell, Peter Angelos, Jung Hwan Baek, Kevin T. Brumund, Feng‐Yu Chiang, Mary Beth Cunnane, Louise Davies, Andrea Frasoldati, Anne Y. Feng, Laszlo Hegedüs, Ayaka J. Iwata, Emad Kandil, Jennifer K
Head & Neck.2022; 44(3): 633. CrossRef - Thyroid Nodule Radiofrequency Ablation: Complications and Clinical Follow Up
James Y. Lim, Jennifer H. Kuo
Techniques in Vascular and Interventional Radiology.2022; 25(2): 100824. CrossRef - American Association of Clinical Endocrinology Disease State Clinical Review: The Clinical Utility of Minimally Invasive Interventional Procedures in the Management of Benign and Malignant Thyroid Lesions
Sina Jasim, Kepal N. Patel, Gregory Randolph, Stephanie Adams, Roberto Cesareo, Edward Condon, Tara Henrichsen, Malak Itani, Maria Papaleontiou, Leonardo Rangel, John Schmitz, Marius N. Stan
Endocrine Practice.2022; 28(4): 433. CrossRef - Efficacy of radiofrequency and laser thermal ablation in solving thyroid nodule-related symptoms and cosmetic concerns. A systematic review and meta-analysis
Roberto Cesareo, Silvia Egiddi, Anda M. Naciu, Gaia Tabacco, Andrea Leoncini, Nicola Napoli, Andrea Palermo, Pierpaolo Trimboli
Reviews in Endocrine and Metabolic Disorders.2022; 23(5): 1051. CrossRef - Comparison of ultrasound-guided radiofrequency ablation versus thyroid lobectomy for T1bN0M0 papillary thyroid carcinoma
Lin Yan, Xinyang Li, Yingying Li, Jing Xiao, Mingbo Zhang, Yukun Luo
European Radiology.2022; 33(1): 730. CrossRef - A systematic review and meta-analysis comparing tumor progression and complications between radiofrequency ablation and thyroidectomy for papillary thyroid carcinoma
Yuan-dong Sun, Hao Zhang, Hai-tao Zhu, Chun-xue Wu, Miao-ling Chen, Jian-jun Han
Frontiers in Oncology.2022;[Epub] CrossRef - RFA and benign thyroid nodules: Review of the current literature
Haris Muhammad, Prasanna Santhanam, Jonathon O. Russell, Jennifer H. Kuo
Laryngoscope Investigative Otolaryngology.2021; 6(1): 155. CrossRef - Radiofrequency ablation and thyroid nodules: updated systematic review
Haris Muhammad, Prasanna Santhanam, Jonathon O. Russell
Endocrine.2021; 72(3): 619. CrossRef - Complications of RFA for Thyroid Nodules: Prevention and Management
Rahul K. Sharma, Jennifer H Kuo
Current Otorhinolaryngology Reports.2021; 9(1): 79. CrossRef - Long-Term Results of Ultrasound-Guided Radiofrequency Ablation of Benign Thyroid Nodules: State of the Art and Future Perspectives—A Systematic Review
Hervé Monpeyssen, Ahmad Alamri, Adrien Ben Hamou
Frontiers in Endocrinology.2021;[Epub] CrossRef - Long-Term Outcomes of Thermal Ablation for Benign Thyroid Nodules: The Issue of Regrowth
Jung Suk Sim, Jung Hwan Baek, Rosaria Meccariello
International Journal of Endocrinology.2021; 2021: 1. CrossRef - Ultrasound-Guided Radiofrequency Ablation Versus Thyroid Lobectomy for Low-Risk Papillary Thyroid Microcarcinoma: A Propensity-Matched Cohort Study of 884 Patients
Lin Yan, Mingbo Zhang, Qing Song, Yukun Luo
Thyroid.2021; 31(11): 1662. CrossRef - Clinical Effects of Microwave Ablation in the Treatment of Low-Risk Papillary Thyroid Microcarcinomas and Related Histopathological Changes
Chenya Lu, Xingjia Li, Xiaoqiu Chu, Ruiping Li, Jie Li, Jianhua Wang, Yalin Wang, Yang Xu, Guofang Chen, Shuhang Xu, Chao Liu
Frontiers in Endocrinology.2021;[Epub] CrossRef - Ultrasound-Guided Thermal Ablation of Thyroid Nodules: Technicalities Progress and Clinical Applications, Especially in Malignant Thyroid Nodules
Enock Adjei Agyekum, Jian-hua Fu, Fei-Ju Xu, Yong-Zhen Ren, Debora Akortia, Qing Chen, Xiao-Qin Qian, Yuguo Wang, Xian Wang
Frontiers in Oncology.2021;[Epub] CrossRef - Comparison Between Radiofrequency Ablation and Microwave Ablation in the Treatment for Benign Thyroid Nodules: a Meta-analysis
Jing Wu, Junguo Liu, Li Liu
Indian Journal of Surgery.2021;[Epub] CrossRef - 2020 European Thyroid Association Clinical Practice Guideline for the Use of Image-Guided Ablation in Benign Thyroid Nodules
Enrico Papini, Hervé Monpeyssen, Andrea Frasoldati, Laszlo Hegedüs
European Thyroid Journal.2020; 9(4): 172. CrossRef - Response: Long-Term Outcomes Following Thermal Ablation of Benign Thyroid Nodules as an Alternative to Surgery: The Importance of Controlling Regrowth (Endocrinol Metab 2019;34:117–23, Jung Suk Sim et al.)
Jung Suk Sim, Jung Hwan Baek
Endocrinology and Metabolism.2019; 34(3): 325. CrossRef
- Comparison of the Therapeutic Efficacy and Technical Outcomes between Conventional Fixed Electrodes and Adjustable Electrodes in the Radiofrequency Ablation of Benign Thyroid Nodules
- Thyroid
- A Comparison of Ultrasound-Guided Fine Needle Aspiration versus Core Needle Biopsy for Thyroid Nodules: Pain, Tolerability, and Complications
- Eun Ji Jeong, Sae Rom Chung, Jung Hwan Baek, Young Jun Choi, Jae Kyun Kim, Jeong Hyun Lee
- Endocrinol Metab. 2018;33(1):114-120. Published online March 21, 2018
- DOI: https://doi.org/10.3803/EnM.2018.33.1.114
- 5,379 View
- 61 Download
- 24 Web of Science
- 22 Crossref
-
Abstract
PDFPubReader ePub
Background To compare pain, tolerability, and complications associated with fine needle aspiration (FNA) versus core needle biopsy (CNB).
Methods FNAs were performed using 23-gauge needles and CNBs were performed using 18-gauge double-action spring-activated needles in 100 patients for each procedure. Patients were asked to record a pain score using a 10-cm visual analog scale and procedure tolerability. Complications and number of biopsies were recorded.
Results The median pain scores were similar for the FNA and CNB approaches during and 20 minutes after the biopsy procedures (3.7 vs. 3.6,
P =0.454; 0.9 vs. 1.1,P =0.296, respectively). The procedure was tolerable in all 100 FNA patients and in 97 CNB patients (P =0.246). The mean number of biopsies was fewer in the CNB group (1.4 vs. 1.2,P =0.002). By subgroup analysis (staff vs. non-staff), no significant difference was detected in any parameter. There were no major complications in either group, but three patients who underwent CNB had minor complications (P =0.246).Conclusion FNA and CNB show no significant differences for diagnosing thyroid nodules in terms of pain, tolerability, or complications.
-
Citations
Citations to this article as recorded by- A comparative analysis of core needle biopsy and repeat fine needle aspiration in patients with inconclusive initial cytology of thyroid nodules
Xuejiao Su, Can Yue, Wanting Yang, Buyun Ma
Frontiers in Endocrinology.2024;[Epub] CrossRef - Assessing Adequacy: A Meta-Analysis of Rapid Onsite Evaluation of Thyroid Nodules
Peter P. Issa, Christina McCarthy, Mohammad Hussein, Aaron L. Albuck, Essam Emad, Mohamed Shama, Krzysztof Moroz, Eman Toraih, Emad Kandil
Journal of Surgical Research.2024; 296: 523. CrossRef - Histology-based and cytology-based needle sampling for targeted next-generation sequencing in the indeterminate thyroid tumors
Chun-Nan Chen, Tsung-Lin Yang
European Archives of Oto-Rhino-Laryngology.2023; 280(8): 3773. CrossRef - Preoperative evaluation of thyroid nodules – Diagnosis and management strategies
Tapoi Dana Antonia, Lambrescu Ioana Maria, Gheorghisan-Galateanu Ancuta-Augustina
Pathology - Research and Practice.2023; 246: 154516. CrossRef - Keloid Development After Fine Needle Aspiration of the Thyroid: A Rare Case and Review of Management Strategies
Shaniah S Holder, Alaerebo S Malvan-iyalla, Sara Arfan, Vimal Basani, Frederick Tiesenga
Cureus.2023;[Epub] CrossRef - Utilidad de la biopsia con aguja gruesa ecoguiada en nódulos tiroideos con punción aspirativa con aguja fina no diagnóstica
R. Cortázar-García, M.D. Martín-Escalante, L. Robles-Cabeza, C. Martínez-Santos
Radiología.2022; 64(3): 195. CrossRef - Thyroid diagnostic modalities (fine needle aspiration and core needle biopsy) with histology correlation: a tertiary centre experience
Sona J Appukutty, Anna Paterson, Nishant S Patel, Adam Duckworth, James Chan, Maria O'Donovan, Alison J Marker
Journal of Clinical Pathology.2022; 75(9): 620. CrossRef - Diagnostic performance of core needle biopsy for nodal recurrences in patients with head and neck squamous cell carcinoma
Ta-Hsuan Lo, Cheng-Ping Wang, Chun-Nan Chen, Tsung-Lin Yang, Pei-Jen Lou, Jenq-Yuh Ko, Yih-Leong Chang, Tseng-Cheng Chen
Scientific Reports.2022;[Epub] CrossRef - The efficacy of incorporating ultrasound-guided core biopsy into the clinical workflow of indeterminate thyroid tumors
Chun-Nan Chen, Min-Shu Hsieh, Yi-Hsuan Lee, Tsung-Lin Yang
Journal of the Formosan Medical Association.2022; 121(10): 2012. CrossRef - A Literature Review of Factors Associated With Pain From Fine Needle Aspiration Biopsy of Thyroid Nodules
Tao Liu, Manisha Tilak, Sara Awad, Joshua Lakoff
Endocrine Practice.2022; 28(6): 628. CrossRef - Usefulness of ultrasound-guided core biopsy in thyroid nodules with inconclusive fine-needle aspiration biopsy findings
R. Cortázar-García, M.D. Martín-Escalante, L. Robles-Cabeza, C. Martínez-Santos
Radiología (English Edition).2022; 64(3): 195. CrossRef - Permanent vocal fold paralysis after ultrasound-guided core needle biopsy of thyroid nodule
Kathrin Zimmerman, Matthew Hoffman, Amalee Smith, C. Blake Simpson
Otolaryngology Case Reports.2022; 24: 100455. CrossRef - Interobserver variability in ultrasound assessment of thyroid nodules
Jaber Alyami, Fahad F. Almutairi, Sultan Aldoassary, Amani Albeshry, Ali Almontashri, Mazen Abounassif, Majed Alamri
Medicine.2022; 101(41): e31106. CrossRef - Usage and Diagnostic Yield of Fine-Needle Aspiration Cytology and Core Needle Biopsy in Thyroid Nodules: A Systematic Review and Meta-Analysis of Literature Published by Korean Authors
Soon-Hyun Ahn
Clinical and Experimental Otorhinolaryngology.2021; 14(1): 116. CrossRef - Hydrodissection: A Novel Approach for Safe Core Needle Biopsy of Small High-Risk Subcapsular Thyroid Nodules
Hojat Ebrahiminik, Hossein Chegeni, Javad Jalili, Rambod Salouti, Hadi Rokni, Afshin Mohammadi, Ali Mosaddegh Khah, Seyed Mohammad Tavangar, Zahra Ebrahiminik
CardioVascular and Interventional Radiology.2021; 44(10): 1651. CrossRef - A Blinded Randomized Trial Comparing 2 Needle Gauges for Fine‐Needle Biopsy of Thyroid Nodules
Christopher M. Shumrick, Jonathan C. Simmonds, Lorna L. Ogden, Cindi A. Snowden, Jagdish K. Dhingra
OTO Open.2021;[Epub] CrossRef - Application of biomarkers in the diagnosis of uncertain samples of core needle biopsy of thyroid nodules
Yan Xiong, Xin Li, Li Liang, Dong Li, Limin Yan, Xueying Li, Jiting Di, Ting Li
Virchows Archiv.2021; 479(5): 961. CrossRef - Diagnostic Efficacy and Safety of Core Needle Biopsy as a First-Line Diagnostic Method for Thyroid Nodules: A Prospective Cohort Study
Min Ji Hong, Dong Gyu Na, Hunkyung Lee
Thyroid.2020; 30(8): 1141. CrossRef - Comparison Between Fine Needle Aspiration and Core Needle Biopsy for the Diagnosis of Thyroid Nodules: Effective Indications According to US Findings
Soo Yeon Hahn, Jung Hee Shin, Young Lyun Oh, Ko Woon Park, Yaeji Lim
Scientific Reports.2020;[Epub] CrossRef - 2019 Practice guidelines for thyroid core needle biopsy: a report of the Clinical Practice Guidelines Development Committee of the Korean Thyroid Association
Chan Kwon Jung, Jung Hwan Baek, Dong Gyu Na, Young Lyun Oh, Ka Hee Yi, Ho-Cheol Kang
Journal of Pathology and Translational Medicine.2020; 54(1): 64. CrossRef - Pathological diagnosis of thyroid nodules based on core needle biopsies: comparative study between core needle biopsies and resected specimens in 578 cases
Yan Xiong, Limin Yan, Lin Nong, Yalin Zheng, Ting Li
Diagnostic Pathology.2019;[Epub] CrossRef - The Significance of Having an Excellent Patient's Comfort with Thyroid Core Needle Biopsy
Pierpaolo Trimboli, Luca Giovanella
Endocrinology and Metabolism.2018; 33(1): 53. CrossRef
- A comparative analysis of core needle biopsy and repeat fine needle aspiration in patients with inconclusive initial cytology of thyroid nodules
Review Article
- Recent Advances in Core Needle Biopsy for Thyroid Nodules
- Chan Kwon Jung, Jung Hwan Baek
- Endocrinol Metab. 2017;32(4):407-412. Published online December 14, 2017
- DOI: https://doi.org/10.3803/EnM.2017.32.4.407
- 5,579 View
- 83 Download
- 28 Web of Science
- 26 Crossref
-
Abstract
PDFPubReader
Core needle biopsy (CNB) was introduced as an alternative diagnostic tool to fine-needle aspiration (FNA), and is increasingly being used in the preoperative assessment of thyroid nodules. CNB provides a definitive diagnosis in most cases, but it sometimes may be inconclusive. CNB has the advantage of enabling a histologic examination in relation to the surrounding thyroid tissue, immunohistochemistry, and molecular testing that can provide a more accurate assessment than FNA in selected cases. Nevertheless, CNB should be performed only by experienced experts in thyroid interventions to prevent complications because CNB needles are larger in caliber than FNA needles. As recent evidence has accumulated, and with improvements in the technique and devices for thyroid CNB, the Korean Society of Thyroid Radiology released its 2016 thyroid CNB guidelines and the Korean Endocrine Pathology Thyroid Core Needle Biopsy Study Group published a consensus statement on the pathology reporting system for thyroid CNB in 2015. This review presents the current consensus and recommendations regarding thyroid CNB, focusing on indications, complications, and pathologic classification and reporting.
-
Citations
Citations to this article as recorded by- Parenchymal microcalcifications in the thyroid gland: Clinical significance and management strategy
Younghee Yim, Hye Sun Park, Jung Hwan Baek, Hyunju Yoo, Jin Yong Sung
Medicine.2023; 102(32): e34636. CrossRef - Strategies for Safe and Effective Core Needle Biopsy of Thyroid Nodules with Macrocalcification
Jae Ho Shin
International Journal of Thyroidology.2023; 16(2): 195. CrossRef - Utilidad de la biopsia con aguja gruesa ecoguiada en nódulos tiroideos con punción aspirativa con aguja fina no diagnóstica
R. Cortázar-García, M.D. Martín-Escalante, L. Robles-Cabeza, C. Martínez-Santos
Radiología.2022; 64(3): 195. CrossRef - Usefulness of ultrasound-guided core biopsy in thyroid nodules with inconclusive fine-needle aspiration biopsy findings
R. Cortázar-García, M.D. Martín-Escalante, L. Robles-Cabeza, C. Martínez-Santos
Radiología (English Edition).2022; 64(3): 195. CrossRef - Effectiveness of core needle biopsy in the diagnosis of thyroid lymphoma and anaplastic thyroid carcinoma: A systematic review and meta-analysis
Vincent Vander Poorten, Nathan Goedseels, Asterios Triantafyllou, Alvaro Sanabria, Paul M. Clement, Oded Cohen, Pawel Golusinski, Orlando Guntinas-Lichius, Cesare Piazza, Gregory W. Randolph, Alessandra Rinaldo, Ohad Ronen, Maria E. Cabanillas, Ashok R. S
Frontiers in Endocrinology.2022;[Epub] CrossRef - A Matched-Pair Analysis of Nuclear Morphologic Features Between Core Needle Biopsy and Surgical Specimen in Thyroid Tumors Using a Deep Learning Model
Faridul Haq, Andrey Bychkov, Chan Kwon Jung
Endocrine Pathology.2022; 33(4): 472. CrossRef - Intraoperative Assessment of High-Risk Thyroid Nodules Based on Electrical Impedance Measurements: A Feasibility Study
Jalil Beheshti Firoozabadi, Reihane Mahdavi, Khosro Shamsi, Hossein Ataee, Abdollah Shafiee, Hojat Ebrahiminik, Hossein Chegini, Parisa Hoseinpour, Afshin Moradi, Narges Yousefpour, Faeze Aghaei, Ali Fardoost, Alireza Ghelichli, Hadi Mokhtari Dowlatabad,
Diagnostics.2022; 12(12): 2950. CrossRef - Assessing the diagnostic performance of thyroid biopsy with recommendations for appropriate interpretation
Su Min Ha, Jung Hwan Baek, Dong Gyu Na, Chan-Kwon Jung, Chong Hyun Suh, Young Kee Shong, Tae Yon Sung, Dong Eun Song, Jeong Hyun Lee
Ultrasonography.2021; 40(2): 228. CrossRef - Update on the Evaluation of Thyroid Nodules
Victor J. Bernet, Ana-Maria Chindris
Journal of Nuclear Medicine.2021; 62(Supplement): 13S. CrossRef - Poorly Differentiated Thyroid Carcinoma: Single Centre Experience and Review of the Literature
Maria Bellini, Marco Biffoni, Renato Patrone, Maria Borcea, Maria Costanzo, Tiziana Garritano, Rossella Melcarne, Rosa Menditto, Alessio Metere, Chiara Scorziello, Marco Summa, Luca Ventrone, Vito D’Andrea, Laura Giacomelli
Journal of Clinical Medicine.2021; 10(22): 5258. CrossRef - Laser Ablation Versus Radiofrequency Ablation for Benign Non-Functioning Thyroid Nodules: Six-Month Results of a Randomized, Parallel, Open-Label, Trial (LARA Trial)
Roberto Cesareo, Claudio Maurizio Pacella, Valerio Pasqualini, Giuseppe Campagna, Mario Iozzino, Andrea Gallo, Angelo Lauria Pantano, Roberto Cianni, Claudio Pedone, Paolo Pozzilli, Chiara Taffon, Anna Crescenzi, Silvia Manfrini, Andrea Palermo
Thyroid.2020; 30(6): 847. CrossRef - 2019 Practice guidelines for thyroid core needle biopsy: a report of the Clinical Practice Guidelines Development Committee of the Korean Thyroid Association
Chan Kwon Jung, Jung Hwan Baek, Dong Gyu Na, Young Lyun Oh, Ka Hee Yi, Ho-Cheol Kang
Journal of Pathology and Translational Medicine.2020; 54(1): 64. CrossRef - Morphological and Molecular Assessment in Thyroid Cytology Using Cell-Capturing Scaffolds
Stefania Scarpino, Silvia Taccogna, Giuseppina Pepe, Enrico Papini, Martina D’Angelo, Federica Cascone, Daniele Nicoletti, Rinaldo Guglielmi, Andrea Palermo, Marcella Trombetta, Alberto Rainer, Chiara Taffon, Anna Crescenzi
Hormone and Metabolic Research.2020; 52(11): 803. CrossRef - European Thyroid Association Survey on Use of Minimally Invasive Techniques for Thyroid Nodules
Laszlo Hegedüs, Andrea Frasoldati, Roberto Negro, Enrico Papini
European Thyroid Journal.2020; 9(4): 194. CrossRef - Malignancy risk of initially benign thyroid nodules: validation with various Thyroid Imaging Reporting and Data System guidelines
Su Min Ha, Jung Hwan Baek, Young Jun Choi, Sae Rom Chung, Tae Yon Sung, Tae Yong Kim, Jeong Hyun Lee
European Radiology.2019; 29(1): 133. CrossRef - Tumor Volume Doubling Time in Active Surveillance of Papillary Thyroid Carcinoma
Hye-Seon Oh, Hyemi Kwon, Eyun Song, Min Ji Jeon, Tae Yong Kim, Jeong Hyun Lee, Won Bae Kim, Young Kee Shong, Ki-Wook Chung, Jung Hwan Baek, Won Gu Kim
Thyroid.2019; 29(5): 642. CrossRef - Risk of Malignancy According to the Sub-classification of Atypia of Undetermined Significance and Suspicious Follicular Neoplasm Categories in Thyroid Core Needle Biopsies
Sae Rom Chung, Jung Hwan Baek, Jeong Hyun Lee, Yu-Mi Lee, Tae-Yon Sung, Ki-Wook Chung, Suck Joon Hong, Min Ji Jeon, Tae Yong Kim, Young Kee Shong, Won Bae Kim, Won Gu Kim, Dong Eun Song
Endocrine Pathology.2019; 30(2): 146. CrossRef - Does Radiofrequency Ablation Induce Neoplastic Changes in Benign Thyroid Nodules: A Preliminary Study
Su Min Ha, Jun Young Shin, Jung Hwan Baek, Dong Eun Song, Sae Rom Chung, Young Jun Choi, Jeong Hyun Lee
Endocrinology and Metabolism.2019; 34(2): 169. CrossRef - Response: Long-Term Outcomes Following Thermal Ablation of Benign Thyroid Nodules as an Alternative to Surgery: The Importance of Controlling Regrowth (Endocrinol Metab 2019;34:117–23, Jung Suk Sim et al.)
Jung Suk Sim, Jung Hwan Baek
Endocrinology and Metabolism.2019; 34(3): 325. CrossRef - A Study on Head and Neck Malignant Lymphoma Diagnosed by Core Needle Biopsy
Keisuke Yamamoto, Tsuyoshi Okuni, Makoto Kurose, Akira Yorozu, Kizuku Owada, Ryoto Yajima, Ayumi Takahashi, Kazufumi Obata, Atsushi Kondo, Kenichi Takano
Practica Oto-Rhino-Laryngologica.2019; 112(9): 609. CrossRef - The Role of Core Needle Biopsy for the Evaluation of Thyroid Nodules with Suspicious Ultrasound Features
Sae Rom Chung, Jung Hwan Baek, Young Jun Choi, Tae-Yon Sung, Dong Eun Song, Tae Yong Kim, Jeong Hyun Lee
Korean Journal of Radiology.2019; 20(1): 158. CrossRef - Safety and Efficacy of Radiofrequency Ablation for Nonfunctioning Benign Thyroid Nodules in Children and Adolescents in 14 Patients over a 10-Year Period
Min Ji Hong, Jin Yong Sung, Jung Hwan Baek, Mi Su Je, Dong Whan Choi, Hyunju Yoo, Sae Jeong Yang, Sang Yu Nam, Eun Young Yoo
Journal of Vascular and Interventional Radiology.2019; 30(6): 900. CrossRef - Reliability of core needle biopsy as a second-line procedure in thyroid nodules with an indeterminate fine-needle aspiration report: a systematic review and meta-analysis
Pierpaolo Trimboli, Luca Giovanella
Ultrasonography.2018; 37(2): 121. CrossRef - The Significance of Having an Excellent Patient's Comfort with Thyroid Core Needle Biopsy
Pierpaolo Trimboli, Luca Giovanella
Endocrinology and Metabolism.2018; 33(1): 53. CrossRef - Ultrasonographic Echogenicity and Histopathologic Correlation of Thyroid Nodules in Core Needle Biopsy Specimens
Ji-hoon Kim, Dong Gyu Na, Hunkyung Lee
Korean Journal of Radiology.2018; 19(4): 673. CrossRef - A Comparison of Ultrasound-Guided Fine Needle Aspiration versus Core Needle Biopsy for Thyroid Nodules: Pain, Tolerability, and Complications
Eun Ji Jeong, Sae Rom Chung, Jung Hwan Baek, Young Jun Choi, Jae Kyun Kim, Jeong Hyun Lee
Endocrinology and Metabolism.2018; 33(1): 114. CrossRef
- Parenchymal microcalcifications in the thyroid gland: Clinical significance and management strategy
Original Article
- Thyroid
- Lack of Associations between Body Mass Index and Clinical Outcomes in Patients with Papillary Thyroid Carcinoma
- Hyemi Kwon, Mijin Kim, Yun Mi Choi, Eun Kyung Jang, Min Ji Jeon, Won Gu Kim, Tae Yong Kim, Young Kee Shong, Dong Eun Song, Jung Hwan Baek, Suck Joon Hong, Won Bae Kim
- Endocrinol Metab. 2015;30(3):305-311. Published online November 26, 2014
- DOI: https://doi.org/10.3803/EnM.2015.30.3.305
- 4,181 View
- 39 Download
- 13 Web of Science
- 14 Crossref
-
Abstract
PDFPubReader
Background Obesity is associated with aggressive pathological features and poor clinical outcomes in breast and prostate cancers. In papillary thyroid carcinoma (PTC), these relationships remain still controversial. This study aimed to evaluate the associations between body mass index (BMI) and the clinical outcomes of patients with PTC.
Methods This retrospective study included 1,189 patients who underwent total thyroidectomy for PTCs equal to or larger than 1 cm in size. Clinical outcomes were evaluated and compared based on the BMI quartiles.
Results There were no significant associations between BMI quartiles and primary tumor size, extrathyroidal invasion, cervical lymph node metastasis, or distant metastasis. However, an increase in mean age was associated with an increased BMI (
P for trend <0.001). Multifocality and advanced tumor-node-metastasis (TNM) stage (stage III or IV) were significantly associated with increases of BMI (P for trend 0.02 and <0.001, respectively). However, these associations of multifocality and advanced TNM stage with BMI were not significant in multivariate analyses adjusted for age and gender. Moreover, there were no differences in recurrence-free survivals according to BMI quartiles (P =0.26).Conclusion In the present study, BMI was not associated with the aggressive clinicopathological features or recurrence-free survivals in patients with PTC.
-
Citations
Citations to this article as recorded by- A Data-Driven Approach to Refine Predictions of Differentiated Thyroid Cancer Outcomes: A Prospective Multicenter Study
Giorgio Grani, Michele Gentili, Federico Siciliano, Domenico Albano, Valentina Zilioli, Silvia Morelli, Efisio Puxeddu, Maria Chiara Zatelli, Irene Gagliardi, Alessandro Piovesan, Alice Nervo, Umberto Crocetti, Michela Massa, Maria Teresa Samà, Chiara Mel
The Journal of Clinical Endocrinology & Metabolism.2023; 108(8): 1921. CrossRef - Potential impact of obesity on the aggressiveness of low- to intermediate-risk papillary thyroid carcinoma: results from a MASTER cohort study
Mijin Kim, Yae Eun Kang, Young Joo Park, Bon Seok Koo, Eu Jeong Ku, June Young Choi, Eun Kyung Lee, Bo Hyun Kim
Endocrine.2023; 82(1): 134. CrossRef - Potential Impact of Body Mass Index on the Clinical Outcome of Papillary Thyroid Cancer After High-Dose Radioactive Iodine Therapy
Jingjia Cao, Xiaolu Zhu, Yaru Sun, Xiao Li, Canhua Yun, Wei Zhang
Frontiers in Endocrinology.2022;[Epub] CrossRef - Nutritional status and follicular-derived thyroid cancer: An update
Luigi Barrea, Marco Gallo, Rosaria Maddalena Ruggeri, Paola Di Giacinto, Franz Sesti, Natalie Prinzi, Valerio Adinolfi, Viola Barucca, Valerio Renzelli, Giovanna Muscogiuri, Annamaria Colao, Roberto Baldelli
Critical Reviews in Food Science and Nutrition.2021; 61(1): 25. CrossRef - Effects of concomitant obesity and diabetes on the aggressiveness and outcomes of differentiated thyroid cancer patients
Onur Elbasan, Dilek Gogas Yavuz
Archives of Endocrinology and Metabolism.2021;[Epub] CrossRef - Association of BMI with Clinicopathological Features of Papillary Thyroid Cancer: A Systematic Review and Meta‐Analysis
R. J. O'Neill, S. Abd Elwahab, M. J. Kerin, A. J. Lowery
World Journal of Surgery.2021; 45(9): 2805. CrossRef - Association Between Aggressive Clinicopathologic Features of Papillary Thyroid Carcinoma and Body Mass Index: A Systematic Review and Meta-Analysis
Aliki Economides, Konstantinos Giannakou, Ioannis Mamais, Panayiotis A. Economides, Panagiotis Papageorgis
Frontiers in Endocrinology.2021;[Epub] CrossRef - Potential Impact of BMI on the Aggressiveness of Presentation and Clinical Outcome of Differentiated Thyroid Cancer
Antonio Matrone, Giovanni Ceccarini, Marianna Beghini, Federica Ferrari, Carla Gambale, Mariaida D’Aqui, Paolo Piaggi, Liborio Torregrossa, Eleonora Molinaro, Fulvio Basolo, Paolo Vitti, Ferruccio Santini, Rossella Elisei
The Journal of Clinical Endocrinology & Metabolism.2020; 105(4): e1124. CrossRef - Correlation between obesity and clinicopathological characteristics in patients with papillary thyroid cancer: a study of 1579 cases: a retrospective study
Huijuan Wang, Pingping Wang, Yu Wu, Xiukun Hou, Zechun Peng, Weiwei Yang, Lizhao Guan, Linfei Hu, Jingtai Zhi, Ming Gao, Xiangqian Zheng
PeerJ.2020; 8: e9675. CrossRef - Lack of association between obesity and aggressiveness of differentiated thyroid cancer
G. Grani, L. Lamartina, T. Montesano, G. Ronga, V. Maggisano, R. Falcone, V. Ramundo, L. Giacomelli, C. Durante, D. Russo, M. Maranghi
Journal of Endocrinological Investigation.2019; 42(1): 85. CrossRef - Mitochondrial DNA haplogroup K as a contributor to protection against thyroid cancer in a population from southeast Europe
Relu Cocoş, Sorina Schipor, Corin Badiu, Florina Raicu
Mitochondrion.2018; 39: 43. CrossRef - The impact of BMI on clinical progress, response to treatment, and disease course in patients with differentiated thyroid cancer
Danuta Gąsior-Perczak, Iwona Pałyga, Monika Szymonek, Artur Kowalik, Agnieszka Walczyk, Janusz Kopczyński, Katarzyna Lizis-Kolus, Tomasz Trybek, Estera Mikina, Dorota Szyska-Skrobot, Klaudia Gadawska-Juszczyk, Stefan Hurej, Artur Szczodry, Anna Słuszniak,
PLOS ONE.2018; 13(10): e0204668. CrossRef - Pretreatment BMI Is Associated with Aggressive Clinicopathological Features of Papillary Thyroid Carcinoma: A Multicenter Study
Shi-tong Yu, Wanzhi Chen, Qian Cai, Faya Liang, Debin Xu, Ping Han, Jichun Yu, Xiaoming Huang
International Journal of Endocrinology.2017; 2017: 1. CrossRef - Associations between body mass index and lymph node metastases of patients with papillary thyroid cancer
Changhua Wu, Liang Wang, Wanjun Chen, Shujuan Zou, Aiju Yang
Medicine.2017; 96(9): e6202. CrossRef
- A Data-Driven Approach to Refine Predictions of Differentiated Thyroid Cancer Outcomes: A Prospective Multicenter Study
Review Article
- Management Guidelines for Patients with Thyroid Nodules and Thyroid Cancer.
- Won Bae Kim, Tae Yong Kim, Hyuk Sang Kwon, Won Jin Moon, Jae Bok Lee, Young Sik Choi, Seok Ki Kim, Sun Wook Kim, Ki wook Chung, Jung Hwan Baek, Byung Il Kim, Do Joon Park, Dong Gyu Na, Jun Ho Choe, Jae Hoon Chung, Hye Seung Jung, Jeong Han Kim, Kee Hyun Nam, Hang Seok Chang, Woong Youn Chung, Soon Won Hong, Suck Joon Hong, Jeong Hyun Lee, Ka Hee Yi, Young Suk Jo, Ho Cheol Kang, Minho Shong, Jin Woo Park, Jong Ho Yoon, Seong Joon Kang, Kwang Woo Lee
- J Korean Endocr Soc. 2007;22(3):157-187. Published online June 1, 2007
- DOI: https://doi.org/10.3803/jkes.2007.22.3.157
- 2,994 View
- 32 Download
- 27 Crossref
-
Abstract
PDF
- No abstract available.
-
Citations
Citations to this article as recorded by- 2023 Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules
Young Joo Park, Eun Kyung Lee, Young Shin Song, Soo Hwan Kang, Bon Seok Koo, Sun Wook Kim, Dong Gyu Na, Seung-Kuk Baek, So Won Oh, Min Kyoung Lee, Sang-Woo Lee, Young Ah Lee, Yong Sang Lee, Ji Ye Lee, Dong-Jun Lim, Leehi Joo, Yuh-Seog Jung, Chan Kwon Jung
International Journal of Thyroidology.2023; 16(1): 1. CrossRef - Identification of Prognostic Biomarkers in Papillary Thyroid Cancer and
Developing Non-Invasive Diagnostic Models Through Integrated Bioinformatics
Analysis
Afsaneh Arefi Oskouie, Mohammad Saeed Ahmadi, Amir Taherkhani
MicroRNA.2022; 11(1): 73. CrossRef - Clinical Implication of World Health Organization Classification in Patients with Follicular Thyroid Carcinoma in South Korea: A Multicenter Cohort Study
Meihua Jin, Eun Sook Kim, Bo Hyun Kim, Hee Kyung Kim, Hyon-Seung Yi, Min Ji Jeon, Tae Yong Kim, Ho-Cheol Kang, Won Bae Kim, Young Kee Shong, Mijin Kim, Won Gu Kim
Endocrinology and Metabolism.2020; 35(3): 618. CrossRef - Establishment of Korean Thyroid Association-10 Years of Development in Internal Medicine
Jae Hoon Chung
International Journal of Thyroidology.2018; 11(1): 7. CrossRef - Ten Years of the Korean Thyroid Association: Achievement and Future
Young Joo Park, Young Shin Song, Ka Hee Yi
International Journal of Thyroidology.2018; 11(1): 1. CrossRef - Decreasing Disease-Specific Mortality of Differentiated Thyroid Cancer in Korea: A Multicenter Cohort Study
Min Ji Jeon, Hee Kyung Kim, Eun Heui Kim, Eun Sook Kim, Hyon-Seung Yi, Tae Yong Kim, Ho-Cheol Kang, Young Kee Shong, Won Bae Kim, Bo Hyun Kim, Won Gu Kim
Thyroid.2018; 28(9): 1121. CrossRef - Eighth edition of tumor-node-metastasis staging system improve survival predictability for papillary, but not follicular thyroid carcinoma: A multicenter cohort study
Mijin Kim, Hye In Kim, Min Ji Jeon, Hee Kyung Kim, Eun Heui Kim, Hyon-Seung Yi, Eun Sook Kim, Hosu Kim, Bo Hyun Kim, Tae Yong Kim, Sun Wook Kim, Ho-Cheol Kang, Won Bae Kim, Jae Hoon Chung, Young Kee Shong, Tae Hyuk Kim, Won Gu Kim
Oral Oncology.2018; 87: 97. CrossRef - Surgical Treatment Guidelines for Patients with Differentiated Thyroid Cancer: The Korean Association of Thyroid and Endocrine Surgeons (KATES) Guidelines Taskforce
Jin-Woo Park, Ki-Wook Chung, Ji-Sup Yun, Hyungju Kwon, Hoon Yub Kim, Kee Hyun Nam, Kyoung Sik Park, Min Ho Park, Ja Sung Bae, Hyun Jo Youn, Kyu Eun Lee, Chi Young Lim, Jin Hyang Jung, Jun-Ho Choe, Lee Su Kim, Su Jung Lee, Jung Han Yoon
Korean Journal of Endocrine Surgery.2017; 17(1): 1. CrossRef - Ultrasound and clinicopathological features of papillary thyroid carcinomas with BRAF and TERT promoter mutations
Soo Yeon Hahn, Tae Hyuk Kim, Chang Seok Ki, Sun Wook Kim, Soohyun Ahn, Jung Hee Shin, Jae Hoon Chung
Oncotarget.2017; 8(65): 108946. CrossRef - Thyroid Fine-Needle Aspiration Cytology Practice in Korea
Yoon Jin Cha, Ju Yeon Pyo, SoonWon Hong, Jae Yeon Seok, Kyung-Ju Kim, Jee-Young Han, Jeong Mo Bae, Hyeong Ju Kwon, Yeejeong Kim, Kyueng-Whan Min, Soonae Oak, Sunhee Chang
Journal of Pathology and Translational Medicine.2017; 51(6): 521. CrossRef - Changes in standardized mortality rates from thyroid cancer in Korea between 1985 and 2015: Analysis of Korean national data
Yun Mi Choi, Won Gu Kim, Hyemi Kwon, Min Ji Jeon, Minkyu Han, Tae Yong Kim, Young Kee Shong, Sang Mo Hong, Eun‐Gyoung Hong, Won Bae Kim
Cancer.2017; 123(24): 4808. CrossRef - Surgical Treatment Guidelines for Patients with Differentiated Thyroid Cancer: The Korean Association of Thyroid and Endocrine Surgeons (KATES) Guidelines Taskforce
Jin-Woo Park, Ki-Wook Chung, Ji-Sup Yun, Hyungju Kwon, Hoon Yub Kim, Kee Hyun Nam, Kyoung Sik Park, Min Ho Park, Ja Sung Bae, Hyun Jo Youn, Kyu Eun Lee, Chi Young Lim, Jin Hyang Jung, Jun-Ho Choe, Lee Su Kim, Su Jung Lee, Jung Han Yoon
Korean Journal of Endocrine Surgery.2017; 17(1): 1. CrossRef - Radiological Justification for and Optimization of Nuclear Medicine Practices in Korea
Byung Il Kim
Journal of Korean Medical Science.2016; 31(Suppl 1): S59. CrossRef - 2016 Revised Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Thyroid Cancer
Ka Hee Yi, Eun Kyung Lee, Ho-Cheol Kang, Yunwoo Koh, Sun Wook Kim, In Joo Kim, Dong Gyu Na, Kee-Hyun Nam, So Yeon Park, Jin Woo Park, Sang Kyun Bae, Seung-Kuk Baek, Jung Hwan Baek, Byung-Joo Lee, Ki-Wook Chung, Yuh-Seog Jung, Gi Jeong Cheon, Won Bae Kim,
International Journal of Thyroidology.2016; 9(2): 59. CrossRef - Sonographic Index for Extrathyroidal Extension of Papillary Thyroid Carcinoma
Ye Won Lee, Tae Hwan Kim, Ho Joon Jang, Min Ju Park, Chang Ki Yeo
Korean Journal of Otorhinolaryngology-Head and Neck Surgery.2015; 58(9): 622. CrossRef - History of Korean Thyroid Association and Recent Debates on Diagnosis and Treatment of Thyroid Cancer in Korea
Kwang Woo Lee
Journal of Korean Thyroid Association.2015; 8(1): 36. CrossRef - RAI Treatment of Distant Metastasis of Thyroid Cancer
Keon Wook Kang
Journal of Korean Thyroid Association.2013; 6(1): 49. CrossRef - Updated guidelines for the diagnosis and management of thyroid nodules
Ka Hee Yi
Journal of the Korean Medical Association.2011; 54(6): 629. CrossRef - Elevated risk of papillary thyroid cancer in Korean patients with Hashimoto's thyroiditis
Kyung Won Kim, Young Joo Park, Eun Hye Kim, So Yeon Park, Do Joong Park, Soon‐Hyun Ahn, Do Joon Park, Hak C. Jang, Bo Youn Cho
Head & Neck.2011; 33(5): 691. CrossRef - Is Comprehensive Neck Dissection a Sole Choice for the Treatment of Recurrent Papillary Thyroid Carcinoma in the Lateral Neck?
Dongbin Ahn, Sun Jae Lee, Sun-Kyun Park, Jin Ho Sohn, June Sik Park
Korean Journal of Otorhinolaryngology-Head and Neck Surgery.2011; 54(1): 62. CrossRef - Revised Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Thyroid Cancer
Ka Hee Yi, Young Joo Park, Sung-Soo Koong, Jung-Han Kim, Dong Gyu Na, Jin-Sook Ryu, So Yeon Park, In Ae Park, Chung-Hwan Baek, Young Kee Shong, Young Don Lee, Jaetae Lee, Jeong Hyun Lee, Jae Hoon Chung, Chan Kwon Jung, Seung-Ho Choi, Bo Youn Cho
Korean Journal of Otorhinolaryngology-Head and Neck Surgery.2011; 54(1): 8. CrossRef - Revised Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Thyroid Cancer
Ka Hee Yi, Young Joo Park, Sung-Soo Koong, Jung-Han Kim, Dong Gyu Na, Jin-Sook Ryu, So Yeon Park, In Ae Park, Chung-Hwan Baek, Young Kee Shong, Young Don Lee, Jaetae Lee, Jeong Hyun Lee, Jae Hoon Chung, Chan Kwon Jung, Seung-Ho Choi, Bo Youn Cho
Endocrinology and Metabolism.2010; 25(4): 270. CrossRef - Can Review of Sonographic Findings Spare Diagnostic Thyroidectomy in Patients with Thyroid Nodules Suspicious of Follicular Neoplasm Cytologically?
Han-Lim Choi, Dong-Ju Kim, Woo-Young Sun, Hyo-Young Yun, Lee-Chan Jang, Jae-Woon Choi, Sung-Young Lee, Ok-Jun Lee, Jin-Woo Park
Journal of the Korean Surgical Society.2010; 79(2): 86. CrossRef - Diagnostic Approaches to Patients with Thyroid Nodules
Ho-Cheol Kang
Journal of the Korean Medical Association.2009; 52(4): 405. CrossRef - Prevalence of Thyroid Nodules Detected by Ultrasonography in Adults for Health Check-up and Analysis of Fine Needle Aspiration Cytology
Jae Hoon Chung
Journal of Korean Endocrine Society.2008; 23(6): 391. CrossRef - The Diagnostic Accuracy of Fine Needle Aspiration Cytology and the Diagnostic Usefulness of Galectin-3 Immunostaining for the Follicular Variant of Papillary Thyroid Carcinoma
Chan-Kwon Jung, Jung-Ha Shin, Hyun-Seung Lee, Ahwon Lee, Eun-Sun Jung, Yeong-Jin Choi, Kyo-Young Lee
The Korean Journal of Cytopathology.2008; 19(2): 160. CrossRef - Prevalence of Thyroid Nodules Detected by Ultrasonography in Adults for Health Check-Ups and Analysis of Fine Needle Aspiration Cytology
Won Jun Kim, Joo Hyong Kim, Dong Won Park, Chang Beom Lee, Yong Soo Park, Dong Sum Kim, Woong Hwan Choi, Tae Wha Kim, You Hern Ahn
Journal of Korean Endocrine Society.2008; 23(6): 413. CrossRef
- 2023 Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules
 First
First Prev
Prev


